
Vitamin D often arrives in the conversation about thyroid health as a quiet variable—one that seems backgrounded until symptoms, lab values, and daily habits begin to line up. For women with thyroid disorders, especially Hashimoto’s thyroiditis, vitamin D may act like a molecular diplomat: negotiating between immune signals and the body’s inflammatory tone. This article guides you through what readers can expect—practical, evidence-informed, and thoughtfully organized—so you can understand how vitamin D fits into the broader endocrine and immunologic landscape.
1) Why Vitamin D Matters in Hashimoto’s Thyroiditis
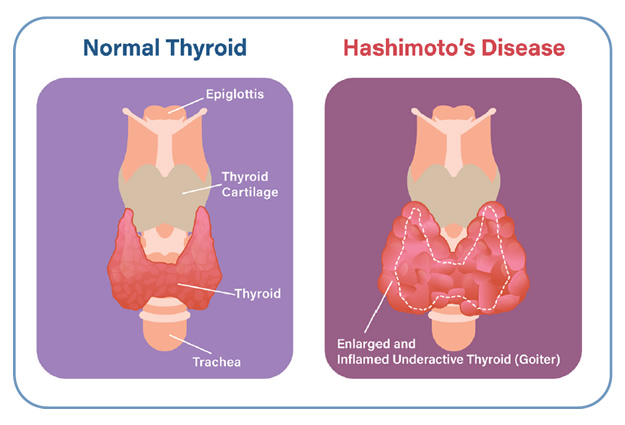
Hashimoto’s thyroiditis is an autoimmune condition where the immune system becomes overzealous, targeting thyroid tissue and gradually impairing hormone production. In that context, vitamin D is frequently discussed for its immunomodulatory potential. Rather than functioning like a classic hormone, vitamin D operates more like a “signal orchestrator,” shaping how immune cells behave, how inflammatory messaging is paced, and how tolerance is maintained.
Women are often central to the discussion because thyroid disorders are more prevalent in females, and life phases—pregnancy planning, postpartum changes, perimenopause, and medication shifts—can all influence vitamin D status. Sun exposure patterns, dietary habits, skin pigmentation, and geographic latitude further affect vitamin D availability. The result can be a chronic tendency toward insufficiency, which may matter when the immune system is already primed toward autoimmunity.
2) Understanding Vitamin D: Hormone, Marker, and Metabolic Actor
Most people measure vitamin D status by checking 25-hydroxyvitamin D in the blood, often abbreviated as 25(OH)D. This is the circulating form that best reflects vitamin D stores. Yet it’s useful to remember: a lab number is not the whole story. Absorption capacity, liver conversion, kidney handling, and the presence of inflammatory states can influence how vitamin D behaves in the body.
Vitamin D works through a receptor found in many tissues, including immune cells. It can influence gene transcription and may help maintain a calmer immunologic environment. Put differently, vitamin D is less about providing “energy” and more about tuning immune regulation—an important distinction for women trying to connect thyroid symptoms with actionable lifestyle steps.
3) Common Symptoms and Why Vitamin D Questions Come Up
Women with Hashimoto’s may experience fatigue, cold sensitivity, weight changes, dry skin, hair thinning, constipation, and mood shifts. Some symptoms overlap with vitamin D deficiency, such as low energy and musculoskeletal discomfort. This overlap can prompt a reasonable question: is vitamin D a contributor, a consequence, or simply an accompanying factor?
It’s often a confluence. Hypothyroidism can influence vitamin D metabolism indirectly through broader metabolic slowdown, while low vitamin D can potentially worsen aches and exercise intolerance. If you notice persistent muscle soreness, weakness, or bone-related discomfort—especially alongside lab-confirmed low vitamin D—addressing vitamin D may become a sensible component of a larger thyroid plan.
4) Lab Testing: What to Ask For and How to Interpret Results
If vitamin D is on your radar, discuss testing with a clinician. The central test is typically 25(OH)D. Depending on your history, additional labs may be considered, such as calcium, phosphorus, and sometimes parathyroid hormone (PTH), especially if deficiency is profound or there are signs of altered mineral metabolism.
Interpretation should be contextual. Values can vary by season, and “normal” ranges may differ across guidelines. Moreover, if you are taking thyroid hormone replacement, optimizing thyroid levels can improve the clarity of symptom patterns. Vitamin D discussion works best when framed as part of coordinated endocrine care rather than a stand-alone fix.
5) Dietary Sources: Building a Vitamin D Pattern, Not a Temporary Plan
Food can contribute meaningfully, but vitamin D is not abundant in many common diets. Fatty fish—such as salmon, sardines, and mackerel—tends to be a reliable option. Egg yolks and certain fortified dairy or plant-based milks can also help. Some cereals and yogurts are fortified as well.
Readers can expect practical guidance here: how to incorporate vitamin D-rich foods without turning meals into a chore, how to pair protein and fats for satiety, and how to remain consistent across busy schedules. A pattern-oriented approach matters because vitamin D intake generally needs continuity to support stable blood levels.
6) Sun Exposure: Helpful, Complex, and Highly Individual
Sunlight can stimulate vitamin D synthesis in the skin. Yet sun exposure is a balancing act: too little reduces vitamin D production, while too much increases risk for skin damage. Lifestyle realities also complicate matters—indoor work, sunscreen habits, seasonal variation, and clothing coverage all affect exposure.
For women, sun exposure strategy can be especially individualized during pregnancy, during dermatologic sensitivities, or when medications increase photosensitivity. The goal isn’t to chase a tanning effect; the goal is to achieve safe, steady vitamin D synthesis when appropriate.
7) Supplements: Choosing Dosing Strategies and Avoiding Common Pitfalls
When dietary intake and sun exposure aren’t enough, supplements are often considered. The most common types are vitamin D3 (cholecalciferol) and vitamin D2 (ergocalciferol). Many women prefer D3 because it tends to be well-studied and widely used, but the right choice should be aligned with clinician guidance and your lab response.
Expect conversations about dosing philosophies. Some people use daily dosing; others use periodic higher-dose regimens under medical supervision. Pitfalls include taking too much without monitoring, using supplements inconsistently, or assuming that “feeling better” means levels have normalized. Vitamin D strategies work best with follow-up labs and a plan that respects absorption variability.
8) How Vitamin D May Influence Immune Activity and Inflammation
Hashimoto’s thyroiditis is not only a thyroid problem; it’s an immune storyline. Vitamin D is frequently discussed because it may modulate immune pathways—potentially affecting inflammatory signaling and the behavior of cells involved in autoimmunity. While the exact degree of benefit can vary from person to person, the mechanistic plausibility is compelling.
Readers can expect a nuanced framing: vitamin D is not a cure-all, and thyroid autoimmunity is multifactorial. However, vitamin D may act as a supportive element, helping the immune system avoid excessive activation. In practical terms, this is where vitamin D feels less like a quick intervention and more like a long-term immunologic “tone-setter.”
9) Interactions with Thyroid Medications and Monitoring Thyroid Levels
Women with Hashimoto’s often take levothyroxine or other thyroid hormone therapies. Vitamin D supplementation should be coordinated with thyroid management. Usually, vitamin D doesn’t directly interfere with thyroid hormone absorption, but overall regimen timing can matter when multiple supplements are used.
Expect guidance on monitoring. Optimizing thyroid hormone levels is foundational. If thyroid levels are not stable, symptoms may persist regardless of vitamin D status. The most coherent approach is parallel: maintain appropriate thyroid therapy while correcting vitamin D insufficiency, then reassess with lab markers over time.
10) Pregnancy, Postpartum, and Life Transitions
Vitamin D needs can be heightened during pregnancy and breastfeeding, and postpartum immune shifts can affect thyroid conditions. Women with Hashimoto’s may already be under closer clinical observation, yet vitamin D status sometimes becomes an overlooked variable amid prenatal appointments and symptom tracking.
Readers can expect careful, safety-minded discussion: supplement decisions during pregnancy should always be clinician-guided, with an emphasis on appropriate dosing, lab monitoring, and avoiding excessive intakes. The aim is not only to support maternal health, but also to contribute to a favorable developmental environment.
11) Safety, Side Effects, and When to Seek Further Evaluation
Vitamin D is generally well-tolerated when dosed appropriately. Still, excessive supplementation can lead to elevated calcium levels and related symptoms such as nausea, constipation, excessive thirst, or confusion. These are uncommon when dosing is reasonable and monitoring is in place, but they are important to know.
Seek further evaluation if fatigue, muscle weakness, or bone pain intensify despite supplementation, or if thyroid symptoms worsen unexpectedly. Severe deficiencies may require tailored regimens, and mineral metabolism anomalies should be addressed rather than guessed.
12) Putting It Together: A Coherent Vitamin D Plan for Women with Hashimoto’s
The most useful takeaway is that vitamin D works best as part of an integrated plan. Start with testing, then build a layered strategy: food first, safe sunlight when feasible, supplementation when necessary, and follow-up labs to confirm response. Meanwhile, keep thyroid hormone management as the anchor.
Short sentence, long impact: consistency beats intensity. When vitamin D is approached thoughtfully—measured, adjusted, and maintained—it can become a stabilizing factor in a complex autoimmune environment. For women navigating Hashimoto’s, that steadiness may translate into fewer “mystery” symptoms, improved resilience, and a more confident sense of control over health.



