



If your vitamin D blood test has come back showing deficiency, the news can feel unsettling—yet it’s also a kind of clarity. A deficiency result is not a life sentence; it’s a map. It tells you that your body’s vitamin D stores are likely insufficient to support normal bone mineralization, immune modulation, and many other physiological processes. The most helpful next step is to interpret the result properly, then move deliberately through a plan that matches your level of deficiency, your risk factors, and your overall health.

1) Read the Result Like a Doctor Would
Vitamin D results are typically reported as 25-hydroxyvitamin D, often abbreviated as 25(OH)D. This is the best marker because it reflects your circulating and stored vitamin D levels. “Deficient” can mean different thresholds depending on the lab and clinical guideline, but the broad idea remains consistent: lower numbers correlate with less available vitamin D activity.
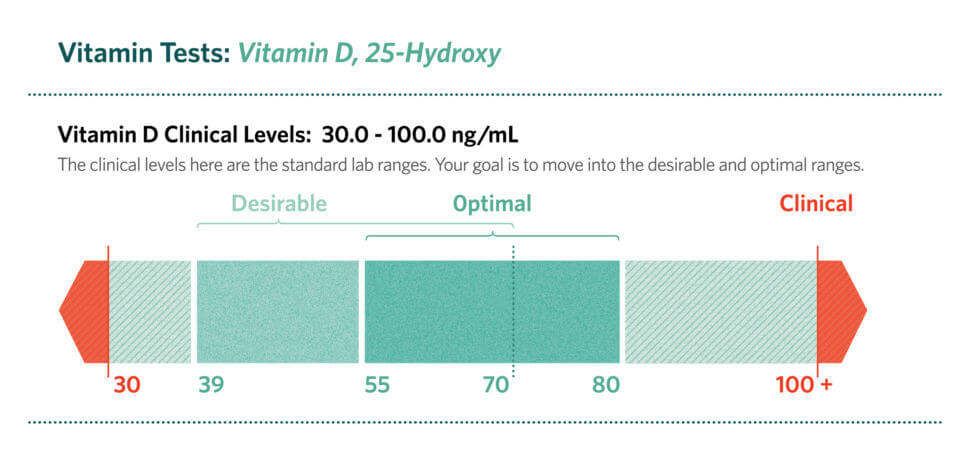
Before changing anything, note the exact value and the reference range printed on your report. Don’t rely solely on the label “low.” The number matters. A level slightly below the cutoff may suggest mild deficiency, while a markedly low value may imply a more urgent need for repletion.
Also check whether your test included related labs such as calcium, parathyroid hormone (PTH), phosphorus, or alkaline phosphatase. Sometimes vitamin D deficiency reveals itself indirectly through elevated PTH, reflecting the body’s attempt to preserve calcium balance.
2) Verify Context: Symptoms, Medications, and Risk Factors
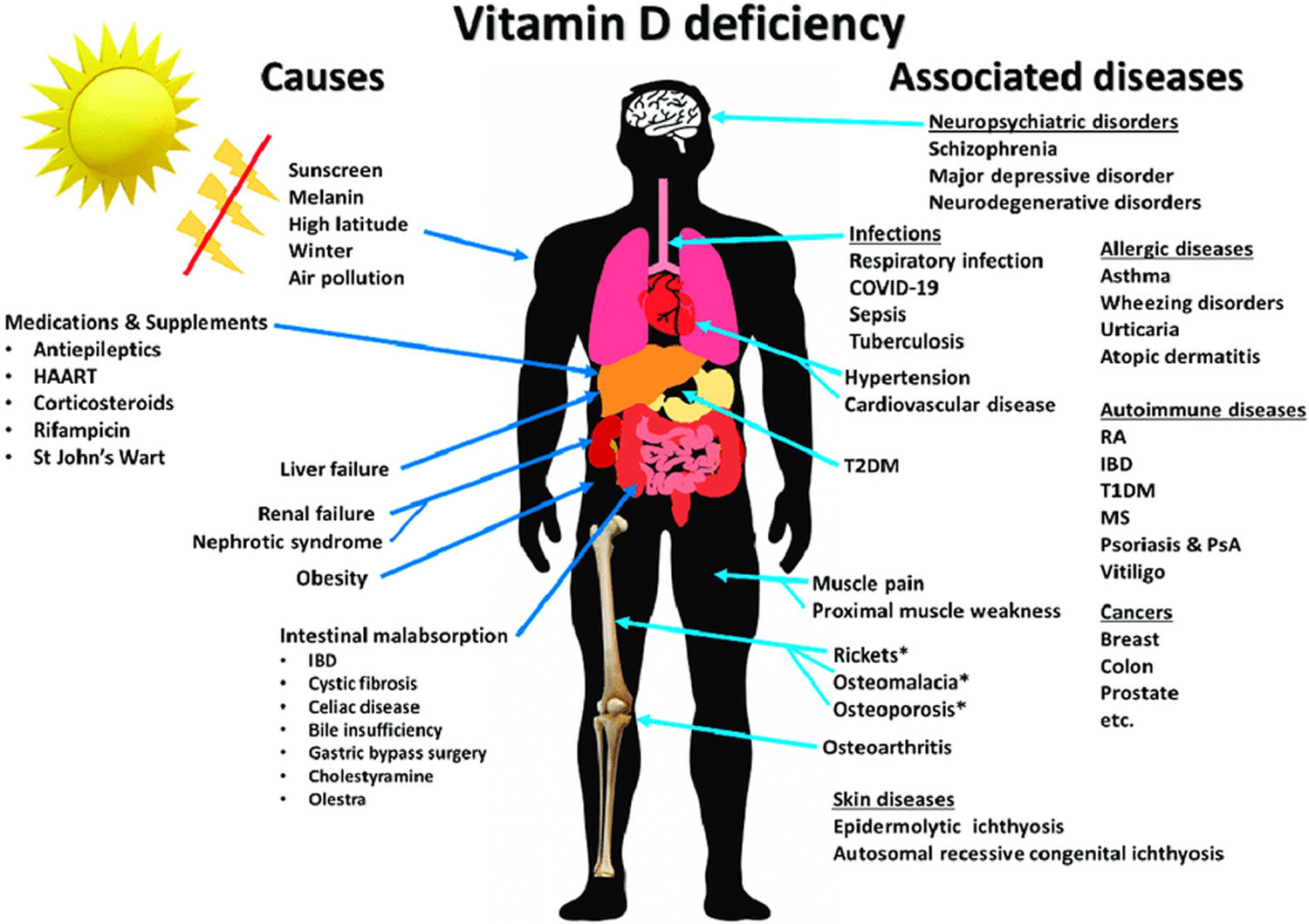
Not everyone feels symptoms from vitamin D deficiency. Some people live normally, while others experience vague musculoskeletal discomfort, fatigue, muscle weakness, or aches that are easy to dismiss. Older adults may be at higher risk due to reduced cutaneous synthesis. People with darker skin can also have lower vitamin D production from sunlight exposure.
Then there are the medication and lifestyle factors. Certain anticonvulsants, glucocorticoids, and weight-loss medications may reduce vitamin D status. Malabsorption syndromes—such as celiac disease, Crohn’s disease, or bariatric surgery outcomes—can prevent absorption even when supplementation is attempted.
Take inventory. Short days, indoor habits, sunscreen overuse (without adequate balancing), limited outdoor activity, and chronic cloud cover can all contribute. The point is not to assign blame; it’s to uncover why the deficiency happened so you can correct the upstream cause.
3) Know the “Why”: What Deficiency Can Affect
Vitamin D supports calcium and phosphate homeostasis, which is central to bone strength. Low vitamin D can contribute to osteomalacia in adults, and in children it can contribute to rickets. Beyond bone, vitamin D is also involved in immune regulation and cellular signaling pathways. That means deficiency can sometimes travel with a broader constellation of health issues.
Think of vitamin D as an orchestrator. It doesn’t act alone; it tunes several systems so they can function in sync. When it’s missing, the body may compensate—often through PTH-driven changes that can gradually stress bones and shift mineral balance.
4) Choose the Right Repletion Strategy (Daily vs. Weekly vs. High-Dose)
Once deficiency is confirmed, treatment generally aims to restore vitamin D stores and then maintain them. There are multiple dosing patterns—daily supplementation, weekly dosing, or sometimes short-term higher-dose regimens. The “best” option depends on how low the level is, how well the person is likely to adhere, and whether malabsorption is present.
Higher-dose regimens are often used for more pronounced deficiency because they can refill stores more quickly. However, this must be done with prudence. Vitamin D is fat-soluble, meaning excess can accumulate. A clinician may monitor trends and adjust dosing to avoid overshooting.
If you’re choosing a supplement, look for vitamin D3 (cholecalciferol) rather than D2 in many common regimens, as D3 is frequently used for repletion. Still, the dosing plan should match your test value and your risk profile.
5) Add Calcium with Intelligence (Not Automatically)
Calcium is a companion, not a replacement. Some people with deficiency also have low dietary calcium. Others may already be taking calcium supplements. The key is to align calcium intake with overall mineral needs, ideally without excessive dosing.
Diet-first strategies—such as dairy, fortified plant milks, yogurt, or calcium-rich leafy greens—can be helpful. But if the diet is insufficient, supplementation may be considered. In cases where blood calcium is abnormal or PTH is elevated, clinicians may recommend targeted supplementation and closer follow-up.
Avoid the temptation to “stack” supplements in a way that creates a new imbalance. Vitamin D repletion can improve calcium absorption, so the body may respond faster than expected in some individuals.
6) Understand Absorption: Take It Like It’s Meant to Be Absorbed
Vitamin D absorbs more efficiently when taken with a meal that contains fat. If you take supplements on an empty stomach, absorption can be less reliable, particularly for people who already have borderline GI absorption or a history of bariatric surgery.
There’s also the question of consistency. A single dose won’t necessarily correct deficiency unless the overall repletion plan is followed. Consider building a routine: a consistent time of day, paired with a meal, and tracked in a way that reduces forgetfulness.
7) Watch for Safety Signals and When to Seek Help
Most people tolerate vitamin D supplementation well when it’s appropriately dosed. Still, the body deserves respect. Signs of too much calcium—such as persistent nausea, constipation, excessive thirst, frequent urination, or confusion—should prompt prompt medical evaluation. True vitamin D toxicity is uncommon, but it can occur with very high, prolonged dosing.
People with kidney disease, a history of kidney stones, or certain endocrine disorders require more careful management. In these contexts, a clinician may adjust dosing and add monitoring for calcium and kidney function.
If you have symptoms that feel severe or unusual—especially bone pain that intensifies or muscle weakness that worsens—don’t treat it as mere discomfort. Take it seriously.
8) Decide What Follow-Up Testing Should Look Like
Re-testing is often recommended to confirm that repletion is working. The timing depends on the dosing strategy. Some clinicians recheck in roughly 8–12 weeks for a reassessment after starting therapy; others tailor timing based on baseline severity and concurrent lab abnormalities.
When you re-test, compare the new value to the original and to the lab’s reference range. A rising number suggests response, but the goal is not only “normalization.” The goal is also stability—sustained adequacy long enough to support bone and metabolic needs.
If your level barely changes despite adherence, malabsorption, incorrect dosing, or interactions may be involved. That’s when investigation becomes valuable rather than frustrating.
9) Maintenance: How to Prevent a Repeat Deficiency
Repletion corrects the deficit; maintenance prevents its return. Long-term adequacy depends on a combination of supplementation, diet, and sunlight exposure where appropriate. For many people, a low maintenance dose becomes the anchor after the initial replenishment phase.
Consider practical lifestyle adjustments. Short, safe exposures to sunlight may help some people, though latitude, skin pigmentation, seasonality, and clothing coverage all matter. In northern climates or winter months, sunlight contribution can be minimal. In those scenarios, regular supplementation can be the more reliable lever.
10) Tailor the Plan: Special Populations and Unique Situations
Pregnancy, breastfeeding, infancy, childhood, and older adulthood each require distinct considerations. Children and adolescents may need careful dosing to support growth and bone development. Older adults may benefit from both vitamin D and fall-risk considerations, since adequate vitamin D status may improve muscle function and balance.
For individuals with malabsorption syndromes, standard dosing may not be enough. Higher doses or alternative forms may be considered. In some settings, clinicians track additional markers such as PTH and calcium to ensure the body’s compensatory mechanisms normalize.
If your deficiency is tied to lifestyle or sunlight exposure, the plan may be simpler. Yet even in that case, personalization is crucial: some people respond strongly to supplementation, while others require additional support to sustain adequate levels.
11) Build a “Vitamin D Routine” That Actually Sticks
Consistency is the quiet hero. A routine reduces decision fatigue and turns supplementation into a predictable behavior. Pair your vitamin D with a meal. Use a pill organizer. Set reminders. Keep a small note in your phone about what you’re taking and when.
Long sentences can be comforting in theory, but life is lived in schedules. The goal is to make adherence effortless. Then, when follow-up blood work arrives, you’ll know whether your plan was effective—because your behavior was measurable.
12) Have the Conversation: Questions to Ask at Your Next Visit
Bring your report and ask direct questions: “What level am I at, and how severe is it?” “What dosing regimen do you recommend for my specific value?” “Should I check calcium, PTH, or kidney function?” “When should I re-test, and what target should I aim for?”
If you’re already taking supplements, ask whether your current dose is sufficient or excessive. If you have GI symptoms or a history of absorption problems, ask what strategy makes sense for your situation.
Lastly, ask about maintenance: “After I’m corrected, what should I take to stay corrected?” That one question often prevents the slow slide back into deficiency.
Vitamin D deficiency can be corrected, but the path is most effective when it’s individualized. Read the numbers carefully, address the “why,” choose a sensible repletion regimen, and confirm progress with follow-up testing. Then build a maintenance routine that supports your health long after the deficiency label fades.




