




Ever wonder if your body is sitting comfortably in the “sweet spot” for vitamin D—or if it’s quietly auditioning for a role it never rehearsed? Here’s a playful question: what if your “normal” lab result isn’t actually the level your cells prefer? The potential challenge is sneaky—many people aim for “adequate” when leading experts often describe “optimal” as a more ambitious target. So let’s untangle the terminology, the numbers, and the reasoning behind what “optimal” really means.

Why “Optimal” Isn’t Just a Bigger Number
When people hear “optimal vitamin D,” they often picture a single magic value. Reality is messier. Vitamin D functions like a backstage manager: it influences calcium balance, immune behavior, muscle performance, and cellular signaling. Because of that, “optimal” becomes a moving target—shaped by study designs, populations, baseline deficiency rates, and how outcomes are measured.
Leading experts generally emphasize that optimal levels should support bone health and broader physiological functions. That doesn’t automatically mean chasing the highest possible number. Extremely high levels can backfire. In other words, “optimal” tends to mean adequate plus protective, not maximal.
How Experts Express Vitamin D: The 25(OH)D Story
Most discussions revolve around 25-hydroxyvitamin D—written as 25(OH)D. This is the circulating form that reflects vitamin D status from sun exposure, diet, and supplements. It’s like the dashboard readout for your vitamin D economy.
Because 25(OH)D is measurable and correlates with vitamin D stores, it becomes the centerpiece of most expert guidance. If you’ve ever had labs that reported “vitamin D, 25-OH,” you’ve seen the number that most clinicians interpret when they discuss optimality.

The Common Ranges: Deficient, Insufficient, and Optimal
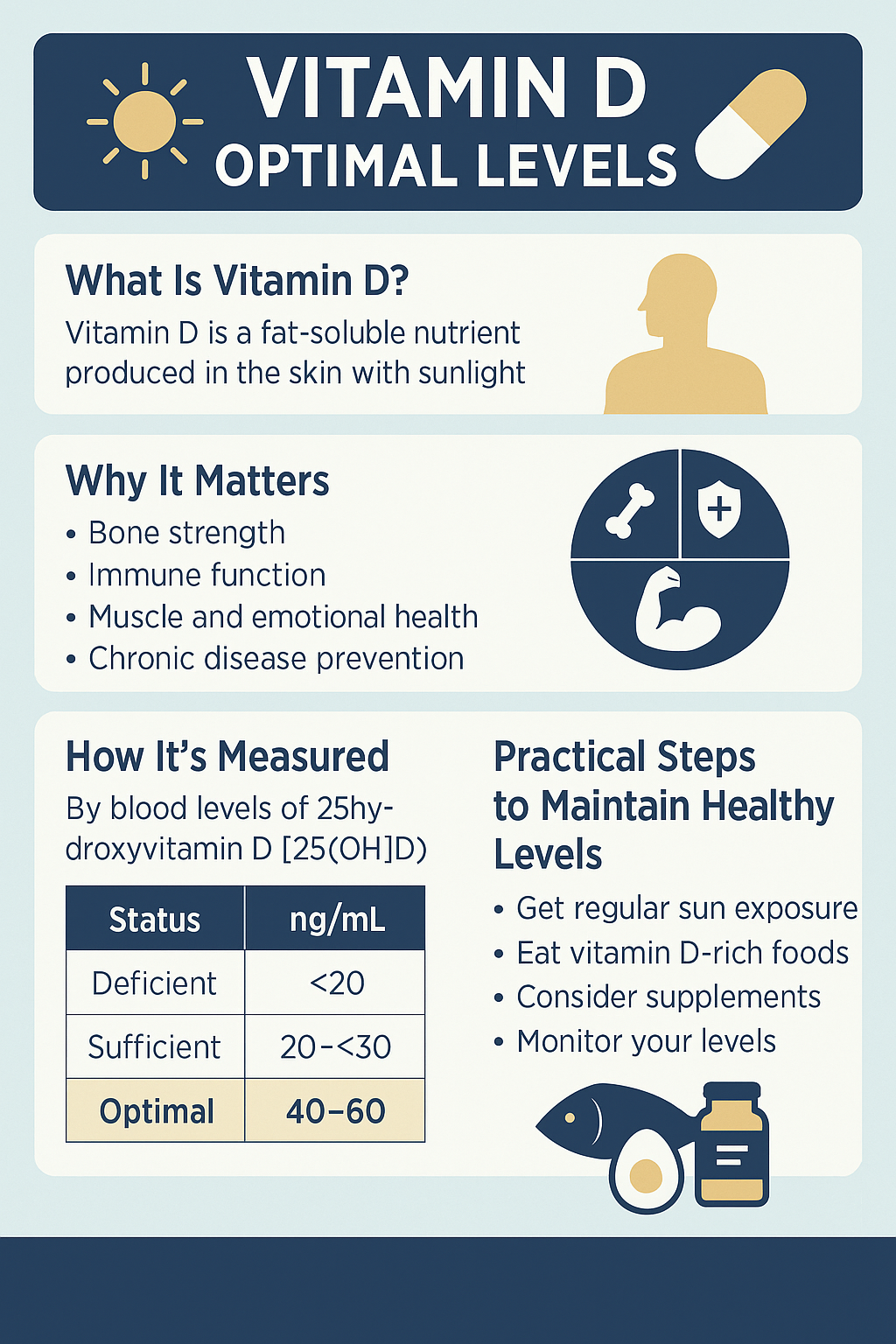
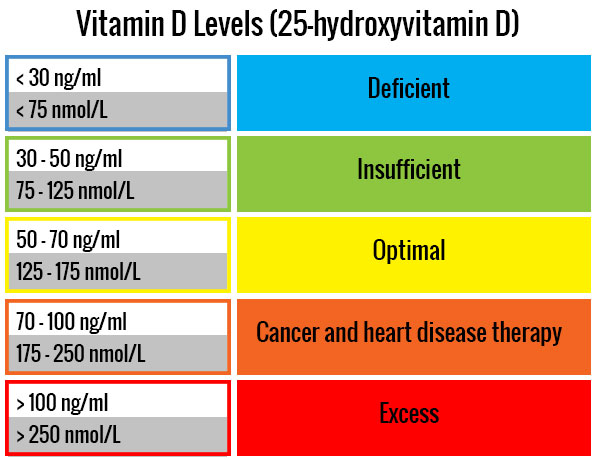
Many lab reports and clinical frameworks categorize vitamin D status into ranges. While exact cutoffs can differ across organizations, a typical pattern looks like this:
Deficient: often below ~20 ng/mL (50 nmol/L).
Insufficient: commonly ~20–30 ng/mL (50–75 nmol/L).
Potentially optimal: frequently around ~30–50 ng/mL (75–125 nmol/L).
Some expert groups suggest that for specific goals—like supporting bone mineral density, reducing fracture risk, or correcting deficiency—aiming for the upper part of the “insufficient” band may be reasonable. But “optimal” is rarely presented as a universal single point. It’s more often a range with intent.
In practice, the “optimal” window is where vitamin D is likely sufficient for normal physiology without edging into territory where toxicity becomes a concern.
Bone Health: The Classic Courtroom for Vitamin D
The strongest historical and clinical justification for targeting an optimal level is bone health. Vitamin D helps regulate calcium absorption in the gut. When vitamin D is too low, calcium uptake can fall, which can push the body to compensate—sometimes by increasing parathyroid hormone (PTH), mobilizing calcium from bones.
In that sense, “optimal” can be framed as: the level at which your body can maintain calcium homeostasis efficiently and keep PTH in a healthier balance. Bone outcomes—like reduced risk of osteomalacia and improved bone mineral density trajectories—often inform where experts draw the “optimal” line.
So, if someone is focused on skeletal outcomes, the rationale becomes less philosophical and more metabolic.
Immune Signaling and the “More Than Bones” Argument
Vitamin D receptors exist in many tissues, including immune cells. That’s why discussions of optimal vitamin D frequently spill into immune modulation. Some experts argue that higher sufficiency levels may better support immune function, especially in populations where deficiency is common or where baseline vitamin D is low due to latitude, skin pigmentation, cultural clothing, or limited sun exposure.
Still, the evidence landscape is uneven. Immune outcomes vary depending on study design, baseline vitamin D status, timing, and individual variability. The upshot: experts may endorse an “optimal” range partly because it’s a pragmatic compromise between biology and measurable clinical endpoints.
Sometimes the goal isn’t to make vitamin D “powerful,” but to make it functionally available for pathways that depend on adequate signaling.
Who Needs a Higher Target?
Here’s where “optimal” starts to feel personal. Several factors can justify aiming toward the upper portion of the sufficiency range:
Baseline deficiency risk: People with little sun exposure or darker skin may require more supplementation to reach the same blood level.
Older age: Skin synthesis declines with age, and absorption patterns may shift.
Body weight and fat distribution: Vitamin D can be sequestered in adipose tissue, potentially reducing circulating levels.
Malabsorption conditions: Celiac disease, inflammatory bowel disease, bariatric surgery, and pancreatic insufficiency can all complicate intake-to-blood conversion.
Medication interactions: Some drugs alter vitamin D metabolism, making monitoring more important.
Leading experts often treat “optimal” as an individualized target guided by clinical context, not a one-size label.
Reading Your Lab Result: Units, Conversions, and Caution
Vitamin D results can appear in either ng/mL or nmol/L. Conversion matters, because confusion here can lead to misguided dosing. As a rough guide: multiply ng/mL by 2.5 to get nmol/L.
Also consider how the test was handled. Timing, sun exposure in the days before testing, supplement habits, and consistency all influence results. A single measurement is a snapshot, not a full biography.
Experts typically recommend that dosing decisions be guided by a combination of the lab value, risk factors, symptoms where relevant, and follow-up testing—especially for those who start with deficiency or require higher doses.
The Upper Boundary: When “Optimal” Turns Risky
Vitamin D is fat-soluble, which means it can accumulate. That’s why expert guidance tends to emphasize not just reaching adequacy, but also avoiding excessive levels. High vitamin D can drive hypercalcemia—an elevation of blood calcium—leading to symptoms such as nausea, constipation, excessive thirst, frequent urination, confusion, and kidney-related concerns.
The key nuance: the threshold for toxicity isn’t simply “a little high.” It’s tied to the interplay between vitamin D and calcium balance, and it’s more likely when vitamin D is supplemented aggressively without monitoring.
In other words, chasing “optimal” without boundaries can become an inadvertent side quest.
How to Maintain “Optimal”: Sun, Food, and Supplements
Sunlight can stimulate vitamin D synthesis, but it depends on season, latitude, cloud cover, skin type, and sunscreen use. Food contributes, though many diets don’t reliably deliver high vitamin D. Fatty fish, fortified dairy or plant alternatives, and certain egg products can help.
Supplements often fill the gap—especially for those at risk of low levels. Many clinicians tailor dosing based on the starting level and risk profile, then recheck labs after a period of consistent intake.
Maintenance is where the long game begins. The “optimal” strategy is usually not a dramatic rescue dose followed by silence. It’s a sustainable routine supported by repeat testing when appropriate.
A Practical Bottom Line: What Leading Experts Often Aim For
So, what vitamin D level is considered “optimal” by leading experts? Most commonly, the concept clusters around reaching at least a sufficiency range—often around 30 ng/mL (75 nmol/L)—with many clinicians considering the 30–50 ng/mL (75–125 nmol/L) window a frequently cited target for broad health considerations.
But the real “optimal” is contextual. It depends on your baseline risk, your health goals (bone health versus general sufficiency), your ability to absorb and convert vitamin D, and how safely you can maintain it.
Here’s the thought to carry into your next lab conversation: the optimal level is not merely a number on paper. It’s the level at which your body is most likely functioning efficiently—with fewer compensations, fewer warning signals, and a smoother metabolic rhythm.



