




Most people first encounter a vitamin D blood test with a practical question: “What exactly am I measuring, and why does it matter?” The deeper answer is that a 25-OH D test is less about a single number and more about a biochemical snapshot—one that quietly reflects sunlight exposure, diet, absorption, liver processing, and even the way the body redistributes this fat-soluble nutrient during times of stress. And yes, it can feel oddly fascinating that a routine lab draw might indirectly illuminate so many invisible processes.

What “25-OH D” Actually Means
A vitamin D blood test labeled 25-OH D measures 25-hydroxyvitamin D, the main circulating form of vitamin D in the bloodstream. This form acts like a well-traveled “intermediate courier,” carrying the vitamin from its origins into the body’s broader metabolism. While vitamin D can enter the body through sunlight-mediated skin production and dietary sources, it does not remain in that initial form for long.
In essence, the test is looking at a stable composite of vitamin D status rather than the fleeting, rapidly changing forms that are harder to interpret. The 25-hydroxy variant is relatively abundant and has a longer half-life, which is why it serves as the customary gauge for overall vitamin D sufficiency.
Think of it as the body’s “running balance” for vitamin D—capturing what’s been accumulated, metabolized, and made available across recent weeks rather than yesterday’s behavior.
Why This Test Is Considered the Best Overview
Vitamin D has multiple stages, and each stage tells a different story. But clinicians tend to prefer 25-OH D because it integrates contributions from several pathways. Sunlight exposure may not be consistent—cloud cover, skin pigmentation, latitude, seasonality, clothing, and even indoor lifestyle patterns can all blunt cutaneous production. Diet can also vary widely. Meanwhile, the body’s internal conversion steps depend on organ function and metabolic demand.
By measuring 25-OH D, the test becomes a practical proxy for the net effect of all those moving parts. It is both retrospective and predictive: retrospective in reflecting recent vitamin D availability, and predictive in informing how much reserve the body likely has for future physiological needs.
There’s a quiet elegance to it. Instead of trying to measure every upstream event separately, the 25-OH D concentration condenses the complexity into one interpretable signal.
Where Vitamin D Comes From Before It Shows Up on the Test
To understand what the blood test measures, it helps to trace the journey. Vitamin D begins as a precursor in the skin. Ultraviolet light converts that precursor into vitamin D3 (cholecalciferol). Alternatively, dietary intake—especially from fortified foods or certain animal sources—can contribute vitamin D2 (ergocalciferol) or D3.
After entry, vitamin D undergoes metabolic transformation. The liver plays a starring role, converting these forms into 25-hydroxyvitamin D. Then, the kidneys and other tissues can further transform it into the hormonally active form, often referenced as 1,25-dihydroxyvitamin D. The key point is that the blood test typically measures the liver-processed intermediate—25-OH D.
That intermediate is why the test can sometimes reveal surprises. A person may appear “healthy” and still show low 25-OH D if sunlight exposure is limited or if metabolic conversion is impaired.
What the Numbers Suggest About Your Body’s Reserve
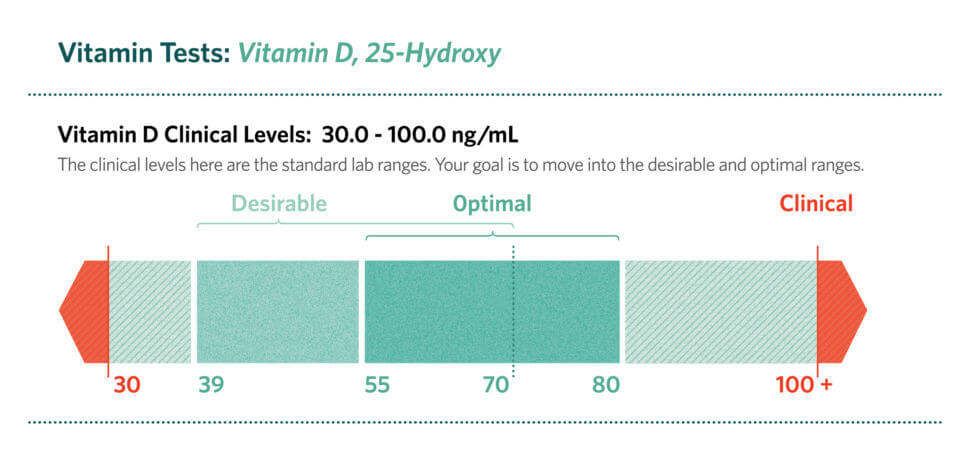
Although reference ranges vary slightly by lab and clinical guideline, vitamin D results are generally interpreted as reflecting sufficiency, insufficiency, or deficiency. The test number matters because vitamin D is not merely a vitamin; it behaves more like a secosteroid hormone that communicates with numerous tissues.
When levels are low, the body may struggle to maintain optimal calcium balance, which is closely linked to bone mineralization. That is why vitamin D testing often surfaces during evaluations for fatigue, bone health concerns, or suspected malabsorption. Low vitamin D status can also correlate with muscle weakness or heightened vulnerability to falls—an observation that frequently prompts clinicians to investigate beyond the obvious.
But deeper still, vitamin D status can reflect broader physiological patterns. It may indicate limited outdoor activity, dietary gaps, inflammatory states, or conditions that alter nutrient handling. A single lab value may therefore function as a subtle mirror held up to lifestyle and biology.
Absorption and Metabolism: The Hidden Contributors
People sometimes assume vitamin D is “simple”: get enough sunlight, and everything will balance. In reality, the pathway from sunlight to usable vitamin D is riddled with potential bottlenecks. Absorption occurs in the gut, and vitamin D is fat-soluble. So if fat absorption is compromised—due to gastrointestinal disorders, certain medications, or bariatric surgery—vitamin D may not be absorbed efficiently even when dietary sources are present.
Similarly, liver function can influence how well vitamin D is converted into 25-OH D. Kidney function also matters downstream for the active hormone form, though the standard blood test still focuses on the more stable intermediate.
This is one reason the test can feel like a detective story. When the result doesn’t match expected lifestyle, it invites questions about malabsorption, medication effects, organ processing, or altered binding and distribution in the blood.
Common Reasons People Get Tested
A vitamin D blood test is often ordered when clinicians suspect deficiency or when a patient has risk factors. These can include minimal sun exposure, darker skin pigmentation (which reduces vitamin D synthesis efficiency), older age, obesity (due to sequestration in adipose tissue), pregnancy or lactation needs, and dietary insufficiency.
It can also be part of a broader evaluation for bone health. Osteopenia, osteoporosis, chronic musculoskeletal pain, or unexplained muscle weakness may trigger measurement. Additionally, certain chronic conditions—particularly those involving the gut, liver, or kidneys—can shift vitamin D status.
Sometimes the test is ordered as a baseline measure during preventive care. Other times it’s used to monitor response after supplementation. Either way, the goal is to translate a number into an informed next step.
How the Blood Sample Is Interpreted in Practice
The test itself is straightforward: a blood draw analyzed for 25-hydroxyvitamin D concentration. However, interpretation benefits from context. A result should be considered alongside symptoms, dietary habits, sun exposure patterns, body mass, medication history, and any known health conditions.
There can be nuance in unit reporting, too. Many labs report either in ng/mL or nmol/L. Conversion is simple, yet overlooking it can lead to confusion. Clinicians also consider whether a test was performed during winter months, after changes in routine, or shortly after starting supplements.
In other words, a lab result is rarely a standalone fact. It’s a data point embedded in a living narrative.
What Happens After Low (or High) Results
When 25-OH D is low, the response often involves lifestyle adjustments and supplementation, followed by reassessment. The strategy can be personalized: some people may benefit from dietary changes and increased safe sun exposure, while others may require higher-dose vitamin D regimens due to malabsorption or limited absorption.
When levels are unexpectedly high, clinicians may evaluate supplementation dosing, adherence patterns, or potential medical contributors. Excessive vitamin D can be associated with elevated calcium levels, which is why follow-up testing may include calcium, kidney function markers, and sometimes parathyroid hormone for a more complete metabolic portrait.
Even here, the fascination persists. The test outcome can prompt a careful recalibration of the body’s mineral economy—how calcium is stored, moved, and utilized.
The Fascination Behind a Simple Test
What makes the 25-OH D measurement captivating is that it sits at the crossroads of environment, physiology, and time. Sunlight offers a seasonal, behavioral input. The liver and gut offer biochemical gates. Muscles, bones, and immune signaling offer downstream effects. Even stress and inflammation may influence how vitamin D-related pathways behave.
In a single blood value, there’s an orchestration of systems: external rays turned into internal messaging, mediated through organs, carried through blood, and interpreted through calcium-related and cellular signaling dynamics.
So when you ask what the test measures, the answer is not only “25-hydroxyvitamin D.” It’s also “the body’s accessible reserve and processing efficiency,” condensed into a number. And behind that number is a remarkably intricate storyline—one that turns a routine test into an intelligible map of how your body is responding to its world.
When to Discuss Results With a Clinician
If you’ve received a vitamin D result—especially if it’s low, high, or surprising—discussion with a healthcare professional can transform the number into action. Consider asking how your level was interpreted for your specific risk profile, whether additional labs are warranted, and what a reasonable target might be in your case.
Because vitamin D status can be influenced by many variables, a thoughtful conversation can clarify whether the result is pointing toward supplementation needs, absorption issues, medication effects, or simply seasonal variation.
Ultimately, a 25-OH D test is both a measurement and an invitation: to look beyond the lab and understand the deeper reasons your body may be signaling for attention.



