Vitamin D is sometimes described as a nutrient, but in osteoporosis care it behaves more like a “metabolic stage light.” It doesn’t build bone by itself; instead, it brightens the biochemical pathways that allow calcium to be absorbed, bone cells to coordinate, and remodeling to proceed with a more harmonious tempo. When vitamin D levels drift too low, the skeleton can start to function like a house with weakened scaffolding—structurally fragile even if the visible walls still appear standing. Setting clear vitamin D level goals turns that uncertainty into a guided plan, where each lab result becomes a compass rather than a cryptic number.
Why Vitamin D Level Goals Matter in Osteoporosis
Osteoporosis is not only about density; it is about the choreography of bone turnover. Osteoblasts and osteoclasts perform their duet under the influence of vitamin D signaling. Without adequate vitamin D, calcium absorption from the gut becomes inefficient, parathyroid hormone (PTH) tends to rise, and the body may compensate by mobilizing calcium from bone. That compensation may feel like an emergency exit—but it comes with structural costs.
That’s why clinicians aim for specific 25-hydroxyvitamin D targets (usually written as 25(OH)D). This marker reflects vitamin D status from sunlight exposure, dietary intake, and supplements. In practice, vitamin D goals are less about achieving perfection and more about preventing the low-vitamin-d “gravity well” that pulls PTH upward and undermines bone mineralization.
Understanding the Key Lab: 25(OH)D and Its Meaning
25(OH)D is the stable circulating form, acting like an “inventory ledger” that records how much vitamin D the body has available. It is different from the active hormone form (calcitriol), which is produced more locally and in response to calcium needs. Because 25(OH)D is the most reliable marker for long-term vitamin D stores, it becomes the anchor for setting level goals.
Metaphorically, if bone health were a library, 25(OH)D is the collection count—not the number of books currently being read. The body can perform short-term borrowing through other mechanisms, but enduring bone strength benefits from consistently adequate “supply.”
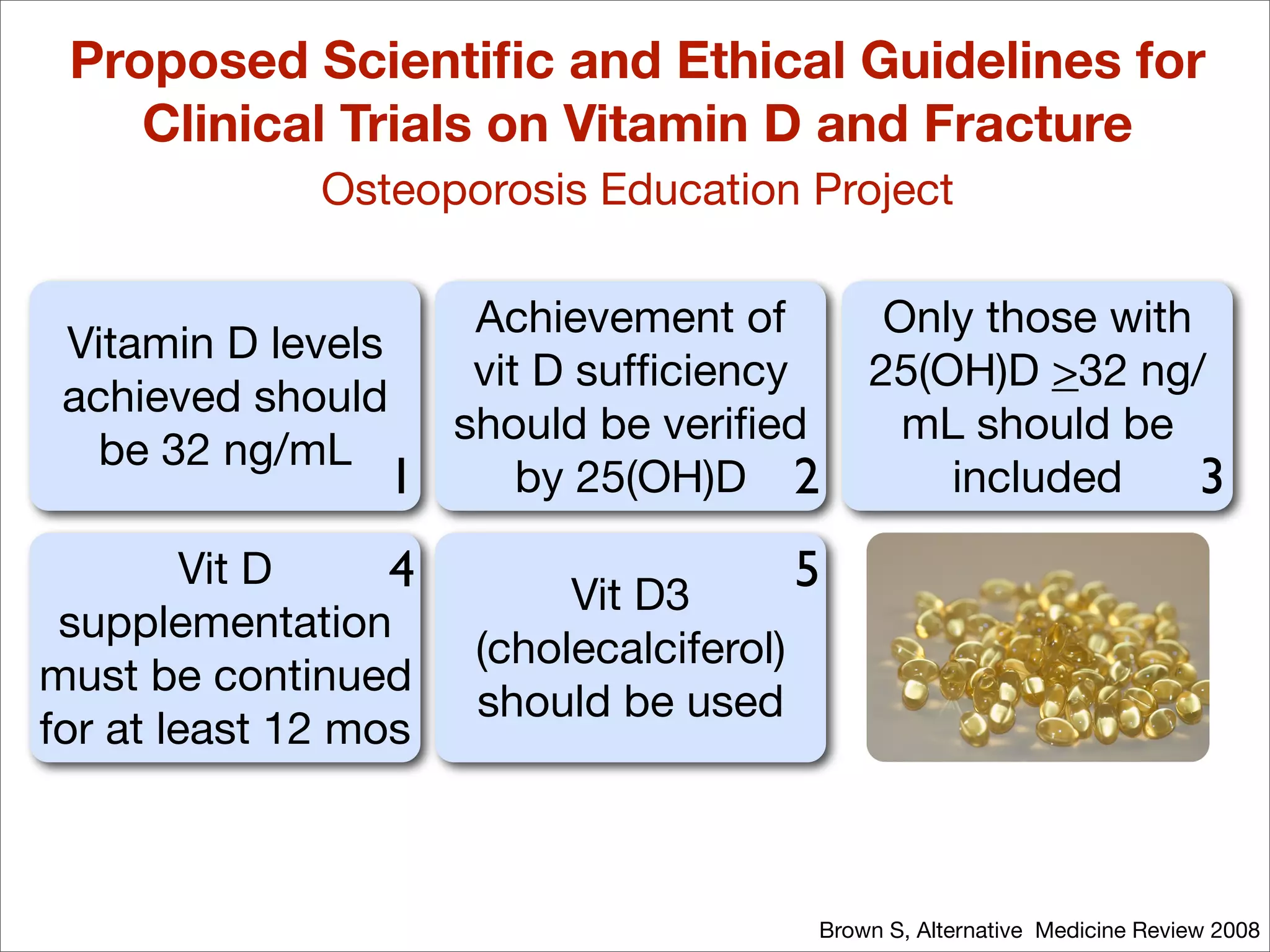
Target Ranges: Practical Vitamin D Level Goals
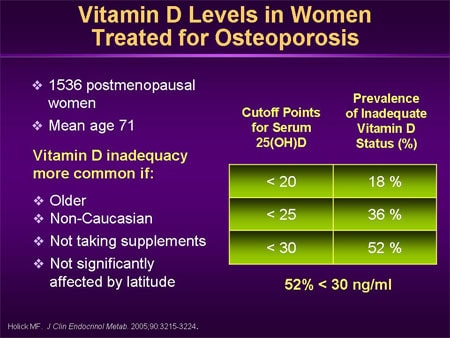
Clinically, many osteoporosis-focused strategies aim for vitamin D sufficiency rather than mere avoidance of deficiency. Common goal thresholds used in practice include:
Sufficiency: approximately 30 ng/mL (about 75 nmol/L) or higher.
Risk reduction: maintaining levels in a range that supports stable calcium handling and avoids secondary hyperparathyroidism.
Older adults and high-risk individuals: often benefit from more assertive targets, since absorption, skin synthesis, and dietary intake can decline with age.
Some patients have “edge-case physiology.” They may have adequate dietary calcium yet still struggle because their vitamin D stores are thin. For those individuals, the goal is to lift 25(OH)D high enough to make calcium absorption and bone mineralization more dependable.
Choosing Goals Based on Risk: Age, Fracture History, and Comorbidities
Not all osteoporosis patients share the same biological climate. Risk stratification matters. A person with recent fragility fracture, limited sun exposure, malabsorption conditions, or chronic kidney disease may require more careful titration and sustained adequacy.
Age can turn sunlight into a rumor rather than a routine. Mobility limitations can reduce outdoor exposure. Medications can also play a role: some therapies affect vitamin D metabolism or calcium balance. The “one-size target” approach is therefore imperfect. The goal should function like a customized key, matching the specific lock of each patient’s risk profile.
How Clinicians Set and Reassess Levels Over Time
Vitamin D management often follows a rhythm: measure, supplement, recheck, then maintain. Initial testing identifies baseline stores. A therapeutic course—whether daily, weekly, or intermittent—raises levels toward the desired range. Then follow-up labs confirm that the body is not only reaching the target but holding it.
Short sentences help mirror the clinical process:
Check. Adjust. Recheck. Continue.
Longer timelines also matter. Bone is living tissue with memory. Improvements in mineralization and remodeling may take months. Meanwhile, PTH and calcium dynamics can shift earlier, offering early clues that the chosen strategy is working.
Supplementation Strategies: Daily vs. Intermittent Regimens
Vitamin D supplementation is typically centered on raising 25(OH)D without overshooting. Dosing varies by baseline level, body weight, absorption efficiency, and kidney function. Daily dosing can offer steady serum concentrations. Intermittent high-dose regimens may be used in select situations, though clinicians often monitor more closely because individual response can be variable.
Consider the difference like this: daily dosing is a slow-cycling irrigation system; intermittent dosing is a seasonal reservoir release. Both can succeed, but the surrounding landscape—dietary intake, sunlight availability, and comorbidities—determines which approach feels more stable.
Calcium Synergy: The Two-Handed Grip of Bone Mineralization
Vitamin D and calcium are often discussed separately, yet osteoporosis management treats them like a two-handed grip. Vitamin D improves intestinal calcium absorption. Calcium provides the raw material for mineralization within the bone matrix.
If vitamin D goals are met but calcium intake is chronically inadequate, the body may still struggle to mineralize effectively. Conversely, high calcium intake without adequate vitamin D can be less efficient, as absorption remains suboptimal. In many plans, supplementation decisions align: either address dietary calcium, add a calcium supplement when needed, or both—always with individualized considerations for kidney stones, dietary habits, and overall cardiovascular context.
PTH as a “Feedback Signal” for Adequacy
Parathyroid hormone can act like a smoke alarm. If vitamin D is insufficient, PTH tends to rise, signaling that the body is trying to maintain calcium availability at the expense of bone. Some clinicians use PTH trends to refine vitamin D goals, especially in patients whose 25(OH)D is borderline or whose calcium absorption is uncertain.
Lower and stable PTH levels often suggest the supplementation strategy is more physiologically aligned. It’s not only about the vitamin D number; it’s about what the body is doing with that number.
Special Populations: Malabsorption, Kidney Disease, and the Elderly
In malabsorption syndromes, vitamin D absorption may be impaired. In those cases, goals still often aim for sufficiency, but dosing strategies may require escalation or alternative formulations. Kidney disease complicates matters because the conversion of vitamin D into its active forms can be impaired, and calcium/phosphate balance must be monitored carefully.
The elderly face a distinct blend of factors: reduced skin synthesis, altered dietary patterns, and a higher probability of concurrent illness. These realities do not invalidate vitamin D goals; they simply demand a more vigilant maintenance plan. The “metabolic stage light” must be kept on, not flickering.
Safety Limits and Avoiding Vitamin D Excess
Vitamin D is powerful, but it is not limitless. Excess can lead to hypercalcemia, renal complications, and vascular concerns in susceptible individuals. That’s why the goal is sufficiency, not maximality. Monitoring is especially important for patients on high-dose regimens, those with kidney disease, or those taking calcium supplements simultaneously.
A well-managed plan treats safety as a steady rail. Patients should be advised not to adjust doses without guidance. Clinicians typically recheck labs after a reasonable interval and adjust to maintain levels within the target window.
Adherence, Lifestyle, and Making Targets Real
Laboratory goals succeed only if they translate into everyday consistency. Adherence can be strengthened with education that feels less like instruction and more like empowerment. Patients often respond to metaphors: vitamin D as a stabilizing conductor, calcium as the instrument, and bone as the orchestra that needs both rhythm and harmony.
Sun exposure can contribute, but it is unpredictable and dependent on latitude, season, skin tone, clothing habits, and skin cancer risk counseling. For many patients, supplementation becomes the reliable route. Diet—fatty fish, fortified dairy or alternatives—supports the plan, even if it rarely replaces supplementation entirely for osteoporosis-level risk.
When to Intensify or Seek Further Guidance
Sometimes vitamin D goals are not reached as expected. Levels may remain low due to inadequate dosing, inconsistent intake, malabsorption, or drug interactions. PTH may stay elevated, and symptoms such as muscle weakness or bone pain may emerge, though these are not specific.
In such scenarios, clinicians may review adherence, re-evaluate dosing, check calcium and renal function, and consider whether additional evaluation is needed for secondary causes of bone loss. The goal remains the same: secure vitamin D sufficiency that supports bone mineralization and reduces fracture risk.
Keeping the Target Over the Long Run
Osteoporosis management is not a single measurement event; it is ongoing stewardship. Vitamin D levels should be maintained within a chosen target range that supports stable calcium metabolism and minimizes compensatory PTH rise. As seasons change, as health status shifts, and as mobility changes, periodic reassessment helps keep the plan aligned with reality.
If vitamin D is the stage light, long-term maintenance ensures the stage remains illuminated. Bone remodeling can then proceed without frantic compensations—more like a well-rehearsed performance than a last-minute improvisation.