
Pregnancy is a season of recalibration. With every trimester, the body rewrites its priorities—supporting fetal skeletal development, modulating immune function, and orchestrating calcium metabolism in a way that can strain even a well-nourished system. Vitamin D sits at the center of that drama, quietly governing absorption and bone health while nudging the endocrine system toward balance. Yet when it comes to dosage, the numbers can feel disorienting. Is 600 IU enough? Is 2000 IU reasonable? And what about 4000 IU? The truth isn’t a single universal answer; it’s a spectrum influenced by baseline status, sun exposure, diet, skin pigmentation, and—most importantly—individual guidance from a clinician.
Why Vitamin D Matters in Pregnancy: More Than “Bone Support”
Vitamin D’s reputation began with bones, but its influence extends well beyond them. During pregnancy, the demand for calcium rises steadily. Vitamin D enables the gut to absorb calcium and helps maintain appropriate serum levels—an essential background condition for fetal growth. It also interacts with immune signaling pathways, which is particularly relevant in pregnancy where immune tolerance must be carefully maintained. This means insufficient vitamin D may show up indirectly: fatigue that feels excessive, musculoskeletal discomfort, or a body that seems to resist optimizing nutrient absorption.
In clinical practice, vitamin D is often discussed through the lens of 25-hydroxyvitamin D—the marker that reflects vitamin D stores. Low stores can be common, especially when sun exposure is limited. Many expectant parents therefore approach dosage as a strategy: not just “taking a supplement,” but steering biochemical reserves toward a target range that supports both mother and baby.
Understanding IU vs. Micrograms: Why Numbers Look Confusing
Before selecting a dose, it helps to translate the language. Nutritional labels may list vitamin D in International Units (IU) or in micrograms (mcg). This matters because people often compare products without realizing they’re not comparing equivalent amounts. A common conversion is that 100 IU of vitamin D equals 2.5 mcg (for vitamin D3). So, as a quick mental scaffold:
600 IU ≈ 15 mcg, 2000 IU ≈ 50 mcg, and 4000 IU ≈ 100 mcg. When guidance is given in mcg but supplements are in IU (or vice versa), misinterpretation becomes easy—like setting a compass with the wrong scale.
To avoid that pitfall, always check the supplement label and confirm the unit of measurement. If the conversion is unclear, a pharmacist or clinician can clarify in a single question.
The Starting Point: Who Might Need 600 IU?
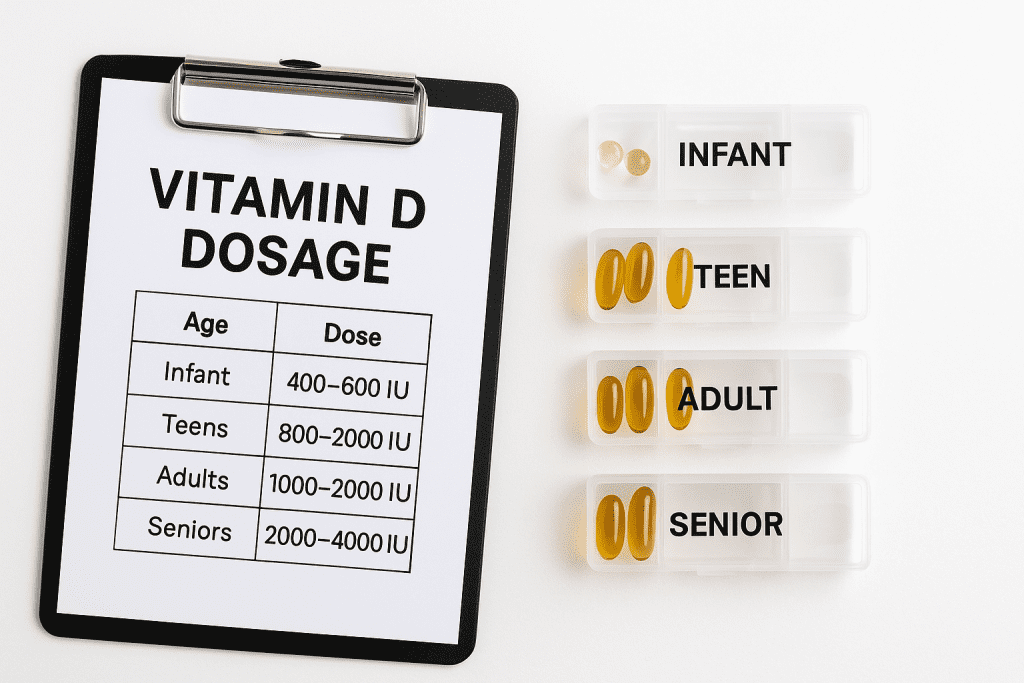
600 IU is often discussed as a baseline intake level, particularly for people who already have reasonable sun exposure, a nutrient-dense diet, and no history of vitamin D insufficiency. Think of 600 IU as a gentle stabilizer—useful when vitamin D stores are adequate or only slightly low.
However, pregnancy can change routines quickly. Nausea, reduced outdoor time, cultural clothing patterns, winter season length, and even geographic latitude can all influence cutaneous vitamin D production. If a person’s baseline vitamin D is unknown, 600 IU may function more like a modest maintenance attempt than a targeted correction.
In practice, 600 IU may be most appropriate when:
• Vitamin D levels are within an acceptable range.
• A clinician has assessed that no aggressive repletion is required.
• Diet and sun exposure are reasonably consistent.
Even then, many clinicians prefer monitoring through bloodwork because pregnancy is too dynamic for assumptions to be perfectly reliable.
Why 2000 IU Often Appears in Prenatal Conversations
2000 IU is frequently chosen because it sits in a “middle lane” between minimal supplementation and more assertive repletion. For many expectant parents, 2000 IU offers a practical balance: enough to meaningfully raise vitamin D stores for those who are insufficient, without immediately approaching the higher end of typical supplemental discussions.
This is especially relevant when the background intake from prenatal vitamins is small. Many prenatal formulas include vitamin D, but the amount may not align with what’s needed in a low-sun environment. Taking additional vitamin D3—under clinician guidance—can help close the gap.
2000 IU may be a particularly sensible option when:
• A recent blood test suggests insufficiency but not severe deficiency.
• Sun exposure is limited due to season, latitude, or lifestyle constraints.
• The goal is steady improvement rather than rapid correction.
That “steady improvement” phrasing matters. Vitamin D is fat-soluble, meaning it accumulates. A gradual course can reduce volatility and help maintain consistent serum levels over time.

When 4000 IU Enters the Picture: Addressing Deeper Insufficiency
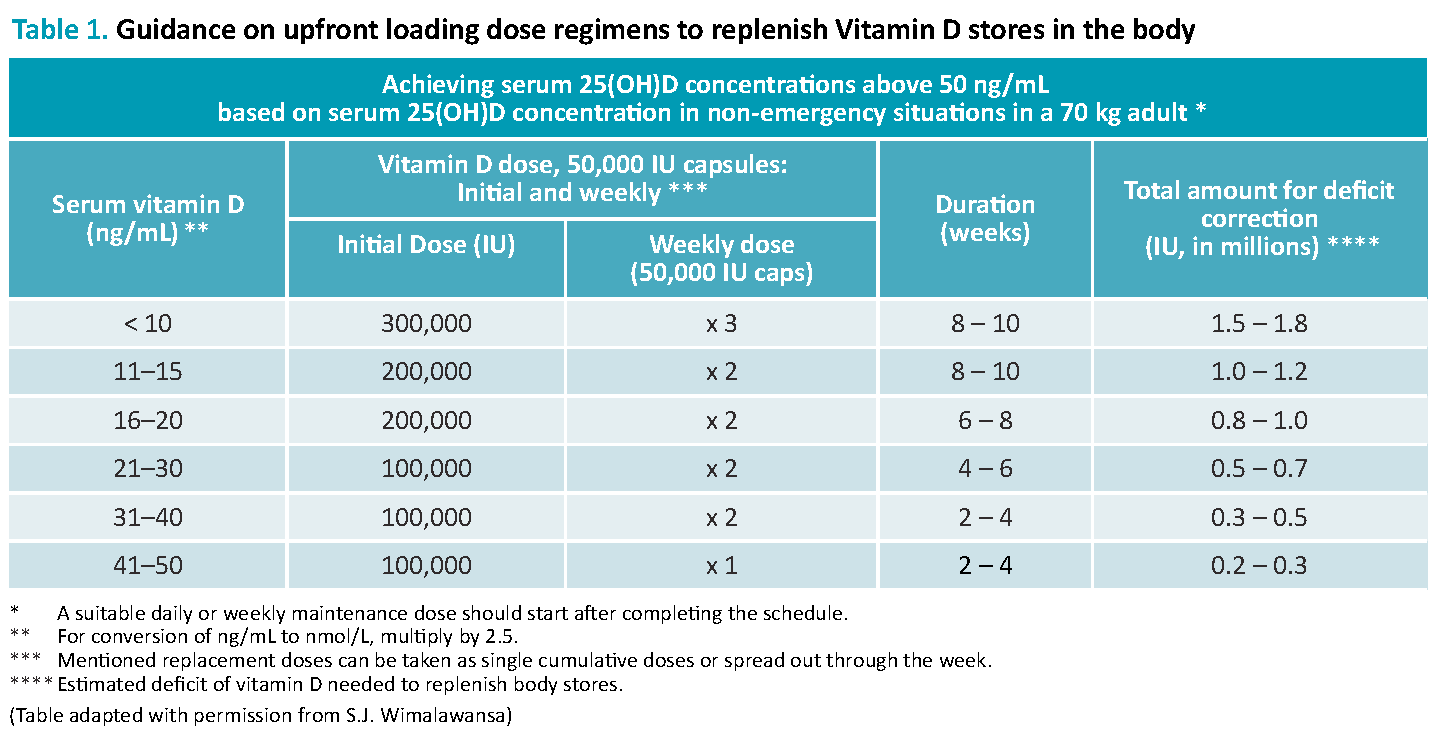
4000 IU is the dosage that often triggers the most questions, and rightly so. Higher doses can be appropriate, but they usually belong to a more measured plan—often anchored by lab results and time-limited repletion rather than long-term casual use.
For individuals with marked deficiency or significantly low baseline levels, 4000 IU may help replenish stores more efficiently. Yet this is not a “set it and forget it” scenario. Because vitamin D can accumulate, clinicians may recommend a specific duration—then recheck levels and adjust.
In other words, 4000 IU can be a surgical instrument rather than a daily blanket. It’s less about boldness and more about precision.
Consider 4000 IU most likely to be used when:
• Bloodwork shows a substantial deficiency.
• There is a clinician-directed repletion strategy.
• Follow-up testing is planned to confirm response and prevent overshooting.
If you hear 4000 IU and feel uneasy, that’s not failure—it’s an invitation to ask the right questions: What was the starting level? What target range are we aiming for? How long will supplementation continue? When will labs be repeated?
Balancing Safety: The Role of Testing, Symptoms, and Clinical Oversight
Safety doesn’t only depend on the dose; it depends on the person. Pregnancy changes physiology, fluid balance, and sometimes how people interpret symptoms. Vitamin D toxicity is uncommon when doses are reasonable and supervised, but it is still a legitimate concern at higher intakes, especially without monitoring. Excessive vitamin D can contribute to elevated calcium, which is not a benign situation.
That’s why clinical oversight matters: it transforms dosage from a guessing game into a controlled intervention. Blood tests can guide decisions more reliably than intuition. In some situations, clinicians may also evaluate calcium status or related parameters.
Symptoms that should prompt conversation include unusual thirst, persistent nausea, constipation that feels extreme, muscle weakness, or confusion. Not all symptoms are vitamin D-related—but dismissing them would be unwise. The pregnancy pathway is already full of sensations; the goal is to distinguish ordinary discomfort from red flags.
Different Types of Content Readers Can Expect: How to Choose What to Trust
When researching vitamin D dosage in pregnancy, readers often encounter three main “content styles,” each with different strengths. Knowing what you’re reading can prevent overreaction or underreaction.
1) Symptom-and-story content. These articles focus on what deficiency can feel like—aching bones, fatigue, and general malaise. Narrative writing can be comforting and memorable, but it may not replace lab-based evidence. Symptoms can overlap with common pregnancy experiences, so this content is best used as a starting prompt, not a final diagnosis.
2) Dosage-and-guideline content. This style lays out numbers, conversions, and typical ranges. It’s practical, but readers should ensure the guidance emphasizes individualization and monitoring. A table can be useful; a plan tailored to your baseline is even more useful.
3) Decision-framework content. The most helpful materials explain how to choose a dose based on test results, risk factors, and follow-up timing. This includes questions about sun exposure, dietary intake, skin tone, and whether the prenatal already includes vitamin D. Decision-framework content also encourages rechecking levels rather than treating vitamin D like a one-time checkbox.
As you compare approaches, look for content that moves from general principles to individualized decision points. Pregnancy deserves that level of specificity.
Practical Next Steps: How to Decide Between 600, 2000, and 4000 IU
Start with what you can control: your lab work, your supplement label, and your conversation with a clinician. If you already have a recent vitamin D level, dosage selection becomes clearer. If you don’t, the first move may be to obtain baseline testing—especially if you have limited sun exposure, darker skin pigmentation, a history of deficiency, malabsorption concerns, or dietary patterns low in vitamin D.
Then align your dosage with the probable objective:
• If aiming for maintenance and levels are adequate, 600 IU may be considered.
• If aiming to correct insufficiency gradually and you have limited sun exposure, 2000 IU is often a pragmatic middle.
• If aiming for repletion after significant deficiency, 4000 IU can be appropriate—usually with a clinician-led timeline and follow-up testing.
Finally, keep the “compound interest” mindset. Vitamin D stores change over time. Reassessment matters. A dose is not merely a number—it’s an ongoing experiment with biochemical feedback.
Conclusion: The Best Dose Is the One That Matches Your Baseline
Choosing between 600 IU, 2000 IU, and 4000 IU during pregnancy isn’t about chasing the highest number or the most fashionable dose. It’s about matching intake to reality: your starting vitamin D status, your risk factors, and your plan for monitoring. For some, 600 IU is a steady maintenance approach. For others, 2000 IU is the bridge that helps reach a healthier reserve. And for a smaller group with more pronounced deficiency, 4000 IU may be a targeted, clinician-guided repletion strategy.
The most confident decisions are never made in isolation. When vitamin D dosage is paired with thoughtful assessment and follow-up, it becomes less of a gamble and more of a reliable ally in pregnancy’s ongoing architectural work.





