
Imagine your skeleton as a library—quietly updating itself day by day. Now imagine three librarians arrive at once: vitamin D, calcium, and strontium. They don’t just work side by side; they operate like a coordinated ensemble. The result can be something more potent than any single nutrient alone: a synergy that supports bone strength, slows decline, and nudges the remodeling process toward resilience.
But here’s a playful question: what happens when one librarian shows up late, or one page of the “bone blueprint” is missing? That’s the potential challenge—bones can’t “borrow” what they never receive.
Why bones behave like living architecture
Bones are not inert scaffolding. They are dynamic mineralized tissue with continual remodeling. Osteoblasts construct; osteoclasts resorb. The balance between these actions determines whether bone density stays robust or gradually erodes.
To keep that equilibrium steady, bones require adequate minerals and biochemical signals. This is where the trio enters the story. Vitamin D helps unlock calcium’s usefulness. Calcium provides the raw building blocks. Strontium appears to influence how the remodeling machinery makes its decisions—quietly altering the conversation between resorption and formation.
Think of remodeling as a renovation cycle: if the supply chain falters (calcium availability) or the construction foreman never arrives (vitamin D signaling), renovation becomes patchy. Add strontium, and the workflow may shift toward preserving more of what’s already been built.
Vitamin D: the conductor that enables calcium’s notes
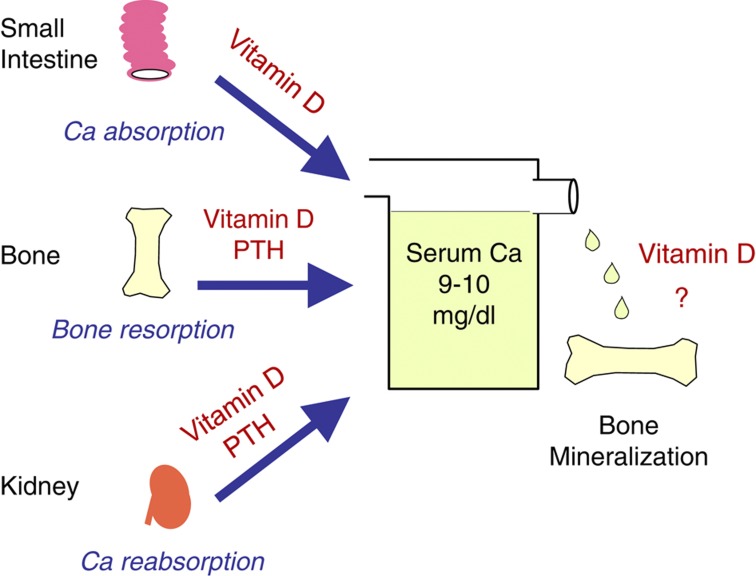
Vitamin D is often described as a “calcium facilitator,” but the role is more elegant than that. It supports intestinal absorption of calcium and helps regulate blood calcium levels. Without sufficient vitamin D activity, calcium can be present in the diet yet fail to translate into bone mineralization effectively.
Vitamin D also participates in endocrine signaling related to bone turnover. When vitamin D status is inadequate, the body may compensate by pulling calcium from bone—subtly reducing the very structure you’re trying to protect.
So the synergy begins with a simple premise: vitamin D improves calcium bioavailability. Better absorption can mean better mineral deposition, and steadier mineralization can mean fewer structural vulnerabilities.
Calcium: the structural mineral that bones demand
Calcium is the cornerstone of hydroxyapatite crystals—the mineral framework responsible for much of bone’s stiffness. When calcium supply is insufficient, bone formation becomes starved, and remodeling can tilt toward net loss.
Dietary calcium contributes directly, but timing and overall intake matter. If daily intake falls short for extended periods, the body’s priorities shift. Hormonal systems attempt to maintain serum calcium, and bone can become the reserve bank.
Here the synergy becomes practical: vitamin D ensures the reserve bank isn’t raided so often, while calcium ensures the remodeling teams have enough material to build. Together they set the stage for structural maintenance.
Strontium: the “behavior modifier” in remodeling
Strontium is chemically akin to calcium, which allows it to interact with bone mineral and remodeling processes. When strontium is incorporated into bone, it may influence crystal properties and the balance between osteoclast activity and osteoblast function.
Rather than acting like a simple mineral replacement, strontium can behave like a conductor for remodeling kinetics. Some evidence suggests strontium can reduce bone resorption and support improved bone microarchitecture.
Microarchitecture is an important word here. Even if bone density looks acceptable on paper, the internal scaffolding—trabecular connectivity and cortical stability—can still be compromised. Strontium’s potential value lies in that nuanced realm.
The synergy: when three inputs create a composite effect
Synergy is not merely “more is better.” It’s the idea that one nutrient improves the effectiveness of another, and the combined effect exceeds individual contributions. Vitamin D improves calcium absorption and utilization. Calcium provides substrate for mineralization. Strontium may alter the remodeling tempo and mineral characteristics.
Picture a construction site. Vitamin D ensures materials arrive and workers can use them. Calcium provides the blocks. Strontium changes the rules so demolition is less frequent and the assembled structure is more durable.
In this composite narrative, the “potential challenge” becomes obvious: if vitamin D is low, calcium can’t fully help. If calcium intake is insufficient, strontium’s benefits may be blunted by a lack of mineral foundation. If strontium exposure isn’t appropriate, the remodeling shift may never occur.
Poses a playful question: are you supplying the whole cast?
Let’s return to the playful question: are you feeding the entire ensemble, or only one star performer?
Many people think of bone health as a single-variable equation: “I take calcium, so I’m covered.” But the body is a multi-step workflow. Calcium is necessary; vitamin D is the gatekeeper; strontium is the modulator. Missing one component can cause the others to underperform.
And here’s the twist: too much of something can also be unhelpful. Bone health strategies need balance. This is why discussing individualized needs with a clinician is more than formality—it’s safety and precision.
A potential challenge: spacing, absorption, and real-world habits
Even well-chosen nutrients can fail to deliver if the routine is inconsistent. Absorption varies. Food matrices influence uptake. Sun exposure and skin physiology affect vitamin D status. Kidney function influences calcium handling and overall suitability of supplementation.
Some people also take multiple supplements at once, which can complicate tolerability. Gastrointestinal discomfort may limit adherence. Fatigue of the routine can quietly reduce consistency, and consistency is a cornerstone of long-term skeletal support.
Consider adopting a “systems approach”: review intake patterns, evaluate lifestyle factors, and ensure that supplementation—if used—aligns with personal health context.
How bone health translates into everyday strength
The ultimate goal is not just numbers on a lab report. It’s the ability to climb stairs without fear, to move with confidence, to avoid fractures that can change a life.
Fracture risk reflects both bone quantity and quality. Bone density is important, but bone quality includes geometry, microarchitecture, and remodeling stability. The synergy of vitamin D, calcium, and strontium aims at multiple layers: absorption and mineral supply, remodeling balance, and structural durability.
When these layers align, bones can become better at handling mechanical stress—the everyday impact from walking, lifting, and even playful missteps.
Support strategies that complement nutrients
Nutrition rarely acts alone. Weight-bearing activity stimulates bone formation and maintenance through mechanotransduction. Resistance training helps preserve both muscle and skeletal support, which can reduce falls—an indirect yet powerful pathway to fracture prevention.
Protein sufficiency matters too. Bone remodeling requires substrates and signaling molecules; inadequate overall nutrition can weaken the rebuilding cycle.
Sleep, sunlight exposure, and smoking status influence endocrine and inflammatory pathways that intersect with bone metabolism. The synergy of nutrients is strongest when lifestyle inputs don’t sabotage the biological machinery.
Images of the bone-remodeling narrative
To visualize how these elements might collaborate, think of a layered process: vitamin D enabling absorption, calcium providing mineral bricks, and strontium subtly reshaping the remodeling choreography.
What to do next: thoughtful, individualized action
The synergy of vitamin D, calcium, and strontium is compelling, but it isn’t one-size-fits-all. Age, hormonal status, dietary patterns, baseline vitamin D level, kidney function, fracture history, and current medications all influence what approach is appropriate.
A sensible next step is to ask targeted questions: Are vitamin D stores adequate? Is calcium intake sufficient from food? Is bone remodeling risk elevated? Does strontium fit your clinical context safely and appropriately?
When the whole cast is present—vitamin D enabling the pathway, calcium supplying the mineral, and strontium potentially adjusting remodeling—you’re not just “taking supplements.” You’re supporting a coordinated biological program designed to keep your skeletal architecture standing tall.



