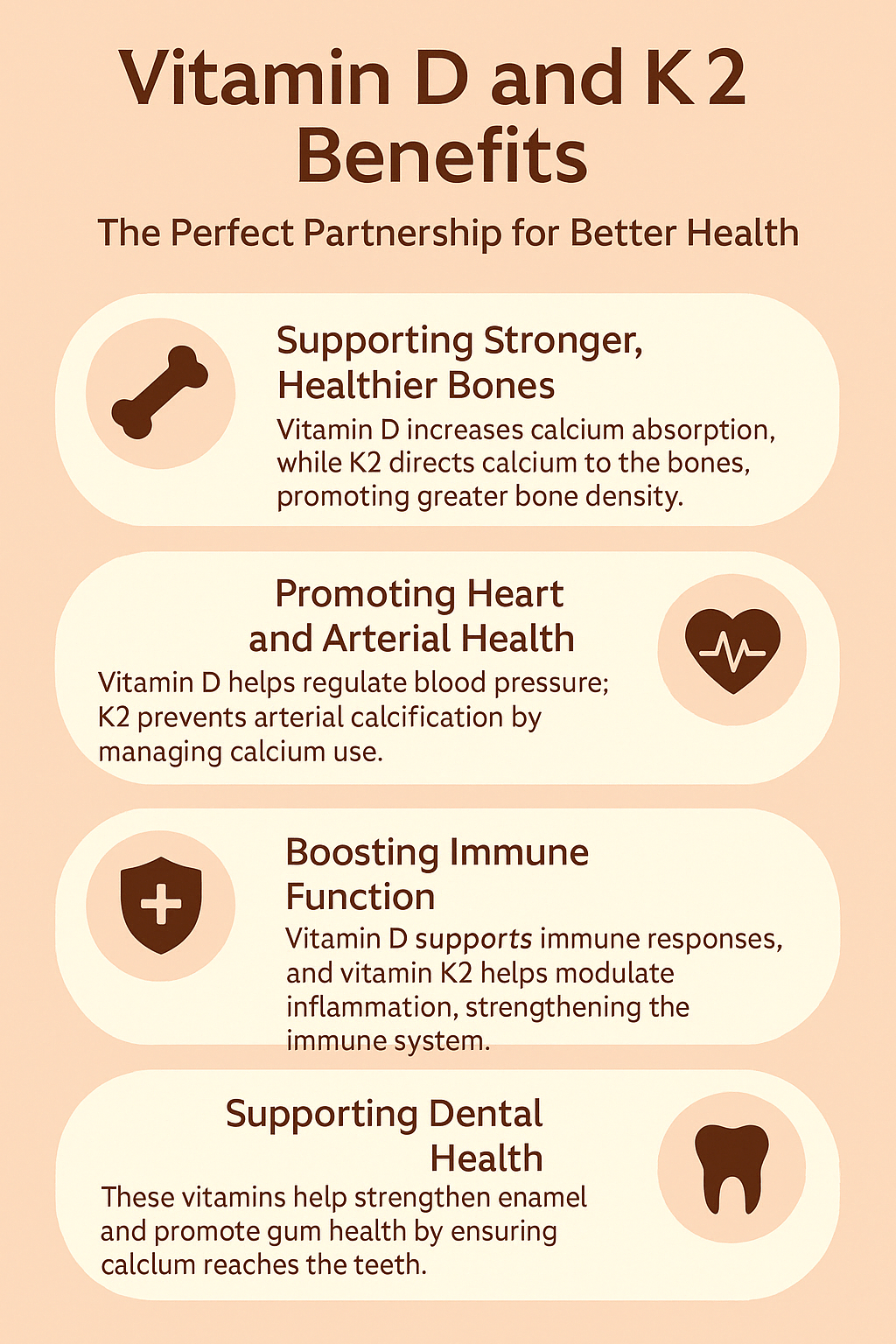
What happens when a “good” vitamin starts behaving like an uninvited guest at the dinner table? Vitamin D is celebrated for bone health, immune modulation, and mood-related pathways—but it can also tip into excess. The tricky part is that vitamin D toxicity is often a silent story at first: symptoms can be vague, the timeline can be long, and the body may keep “going” even as calcium levels climb. Here’s where vitamin K2 enters like a careful conductor—helping channel calcium to the places it belongs, and away from where it shouldn’t. And yes, it’s worth exploring the potential challenge: could supplementing vitamin D without attention to K2 be like adding more paint to a wall without checking the primer?
Why Vitamin D Can Become Too Much
Vitamin D, particularly in its active signaling forms, orchestrates calcium and phosphate homeostasis. When intake is moderate, this orchestration supports mineralization and skeletal integrity. But when vitamin D accumulates—whether from aggressive supplementation, high baseline stores, or prolonged exposure—the downstream effect can be a hypercalcemic crescendo.
Vitamin D toxicity is often linked to elevated calcium (hypercalcemia) and, in some cases, elevated urinary calcium (hypercalciuria). That can set the stage for dehydration, nausea, constipation, fatigue, and confusion. In more severe scenarios, calcium can precipitate in soft tissues. This is where the story becomes urgent: the goal isn’t just “more vitamin D.” The goal is balanced mineral flow, with calcium guided toward bone rather than scattered into tissues.
Calcium: The Double-Edged Sword
Calcium is not the villain—far from it. It is essential for nerve transmission, muscle contraction, vascular function, and cellular signaling. The problem arises when calcium rises beyond physiologic need. Then, the body’s buffering systems can become overwhelmed.
Think of calcium like water pressure. Normal pressure energizes systems. But excessive pressure strains pipes and fixtures. Similarly, excessive calcium can contribute to kidney stress and may correlate with vascular calcification risk. The body has protective mechanisms, yet these mechanisms require the right molecular “keys” to operate effectively.
Where Vitamin K2 Fits Into the Equation
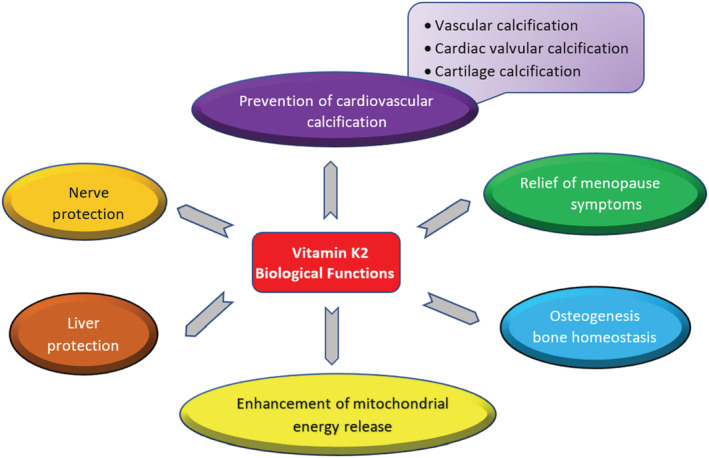
Vitamin K2 is often described as a calcium “allocator.” That phrasing isn’t just poetic—it reflects biochemical reality. Vitamin K serves as a cofactor for enzymes that activate specific proteins involved in mineral regulation.
One of vitamin K2’s best-known roles is supporting the activation of matrix Gla protein (MGP), a protein that helps inhibit calcification in soft tissues. In parallel, vitamin K2 supports osteocalcin activation, a protein involved in bone mineralization. So vitamin K2 doesn’t merely “reduce” calcium. It helps determine calcium’s destination and timing.
If vitamin D increases calcium absorption from the gut and mobilizes mineral signaling, K2 helps provide the molecular escort service—keeping calcium on-course toward bone and discouraging errant deposition.
The Vitamin D Toxicity Concern: It’s Not Only Calcium, It’s Location
Classic discussions of vitamin D excess focus on lab values like 25(OH)D and calcium. But the more nuanced question is: where does calcium go? The body can tolerate calcium increases to a point, especially when regulation systems are functioning and when mineralization demands are present.
Vitamin K2 becomes especially relevant when dietary patterns and gut microbiome factors are suboptimal, or when supplementation stacks without monitoring. Some people may absorb ample vitamin D but have limited K2 intake, particularly if the diet is low in K2-rich foods. In such cases, calcium may rise while the “brakes” on soft-tissue calcification are less effectively engaged.
Mechanisms in Plain Language (and a Little Oddly Specific)
Mechanistically, the story centers on vitamin K-dependent carboxylation of mineral-regulating proteins. Without sufficient K activity, those proteins may remain under-activated. The consequences can be subtle at first: a system designed to “stamp” calcium into appropriate structures doesn’t perform at full efficiency.
Vitamin D pushes calcium absorption and utilization signals. Vitamin K2 helps “complete” the protein instructions that govern mineral placement. When K2 is present, the body is better equipped to maintain a fine-grained balance. When K2 is insufficient, calcium may still rise—but the choreography becomes less precise.
This is why vitamin D toxicity should be treated as more than an isolated vitamin problem. It’s a systems question: absorption, transport, activation, and deposition must all harmonize.
Soft Tissue Calcification: The Quiet Risk
Soft tissue calcification is often described as a long-term process. That’s partly true. Yet the groundwork can begin with biochemical shifts. When calcium is elevated and regulatory pathways are compromised, the environment becomes more conducive to deposition in places like blood vessels and other soft tissues.
Vitamin K2’s support of MGP-mediated inhibition is therefore a compelling protective angle. It doesn’t mean vitamin D excess will automatically cause calcification—biology rarely behaves with simplistic inevitability. But it does mean that adequate K2 may improve resilience by strengthening anti-calcification defenses.
In a playful analogy, imagine vitamin D as the sun that warms the soil. Great. But if you don’t have enough gardeners (K2-dependent enzymes) to steer growth into the intended beds (bone) and prevent sprouting where it shouldn’t (soft tissues), the garden can become chaotic.
Osteocalcin and Bone: The “Right Destination” Advantage
Bone mineralization is not merely a passive storage process. It’s an active remodeling landscape. Vitamin K2 supports osteocalcin activation, which is associated with binding calcium to the bone matrix. In practical terms, this supports the idea that vitamin D’s mineral-boosting effects are most beneficial when K2-dependent bone-related proteins are functioning well.
Here’s the challenge embedded in the phrase “prevent vitamin D toxicity.” Preventing toxicity isn’t only about preventing high calcium. It’s also about making sure calcium has meaningful metabolic routes. Bone remodeling needs the right molecular conditions, and K2 helps supply some of those conditions.
Do You Need Both? A Balanced Supplementation Strategy
For many people, vitamin D supplementation is used to correct deficiency or maintain sufficiency. That’s reasonable. But the most thoughtful approach considers downstream mineral balance. K2 may be relevant, especially for individuals using higher vitamin D doses, those with limited dietary K2 intake, or those with risk factors for impaired calcium regulation.
It’s also wise to consider the role of vitamin K antagonists. Medications such as warfarin affect vitamin K recycling and can alter vitamin K-dependent enzyme activity. In those cases, K2 supplementation decisions require medical guidance.
Perhaps the best mindset is not “stack and hope,” but “coordinate and verify.” Use dietary assessment and, when appropriate, lab monitoring to understand what’s happening inside rather than guessing.
Signs You Should Reassess Your Vitamin D Plan
Vitamin D toxicity risk isn’t something to “notice later.” Early signals can include increased thirst, frequent urination, weakness, nausea, constipation, and cognitive fog. These are not exclusive symptoms, but they are signals that mineral balance might be drifting.
If someone is supplementing vitamin D and experiences such changes—especially in combination with elevated calcium on labs—it’s prudent to reassess. The goal becomes recalibrating intake and supporting the body’s regulation rather than doubling down.
A potential challenge worth considering: lifestyle changes can alter absorption and requirements. Seasonal variation, body weight changes, and shifts in dietary fat intake can influence vitamin D status. Without periodic reassessment, a dose that once fit may become excessive.
Imaging the Whole System: Diet, Gut Microbiome, and Timing
Vitamin K2 is found in certain animal-based foods and fermented sources, while the microbiome can contribute variably to K2-related pathways. Diet patterns—plus fat intake—can influence absorption of both vitamin D and K2. Timing can also matter. Some people take supplements alongside meals for better absorption, while others prefer separate schedules. Individual responses vary.
Rather than treating supplements as isolated ingredients, treat them as parts of a mineral orchestration. Vitamin D enhances calcium availability. Vitamin K2 helps enforce the “destination rules.” Without both, the orchestra may play loudly but not perfectly in tune.
How to Think About Prevention: Evidence-Informed Caution
Prevention is not a guarantee. It is a strategy. A responsible strategy includes appropriate dosing of vitamin D, awareness of contraindications and interactions, and consideration of calcium intake and related lab markers when indicated.
Vitamin K2 is a plausible supportive factor in the context of calcium regulation, particularly when vitamin D is elevated through supplementation. Yet the most important safeguards remain monitoring, individualized guidance, and avoiding extreme dosing. If vitamin D is the “boost,” vitamin K2 may function as the “stabilizer”—helping prevent an overactive mineral signal from turning into a misplaced mineral problem.
If you’re pairing vitamin D with a thoughtful plan rather than a blind one, you’re already ahead. And the best question to ask isn’t only “Do I have enough vitamin D?” It’s also “Am I guiding calcium wisely—and protecting against the consequences of imbalance?”