
Muscle loss rarely announces itself with fanfare. It arrives like a quiet corrosion—subtle at first, then unmistakable. When semaglutide enters the story, the conversation often turns to weight, appetite, and metabolic calm. Yet beneath that familiar narrative lies a more delicate subplot: the potential relationship between semaglutide, vitamin D status, and the body’s ability to preserve—or gradually relinquish—muscle. Think of your muscles as a suspension bridge: weight-bearing, posture-stabilizing, and dependent on the right scaffolding. Vitamin D can be one such scaffold, while semaglutide may alter the environmental conditions that determine how well the bridge holds.
Semaglutide and the “hidden physics” of muscle maintenance
Semaglutide is often described as a medication that helps reduce appetite and improve glycemic control. But for muscle, the more consequential factor is what happens when overall energy intake shifts. Muscles are metabolically expensive tissues; they don’t simply “sit there.” They bargain for resources constantly. When calories tighten—especially over months—the body reallocates. Part of the reallocation can be beneficial, especially if excess fat is reduced. However, muscle is not a negotiable luxury. It is functional architecture: force production, glucose disposal, thermogenesis, and resilience during aging.
Here is the intriguing metaphor: semaglutide can be like turning down the thermostat in a workshop. The tools still exist, but if raw materials and signals change, the maintenance schedule changes too. The question becomes whether the body receives enough “maintenance instructions”—nutrients, sunlight-derived hormones, resistance stimuli—to keep muscle tissue from being used as spare parts.
Muscle preservation often depends on two pillars: mechanical tension (strength training) and biochemical adequacy (micronutrients, protein, and vitamin D). If either pillar weakens, muscle can become collateral damage in the broader weight-loss plot.
Vitamin D: not a “bone supplement,” but a muscle conductor
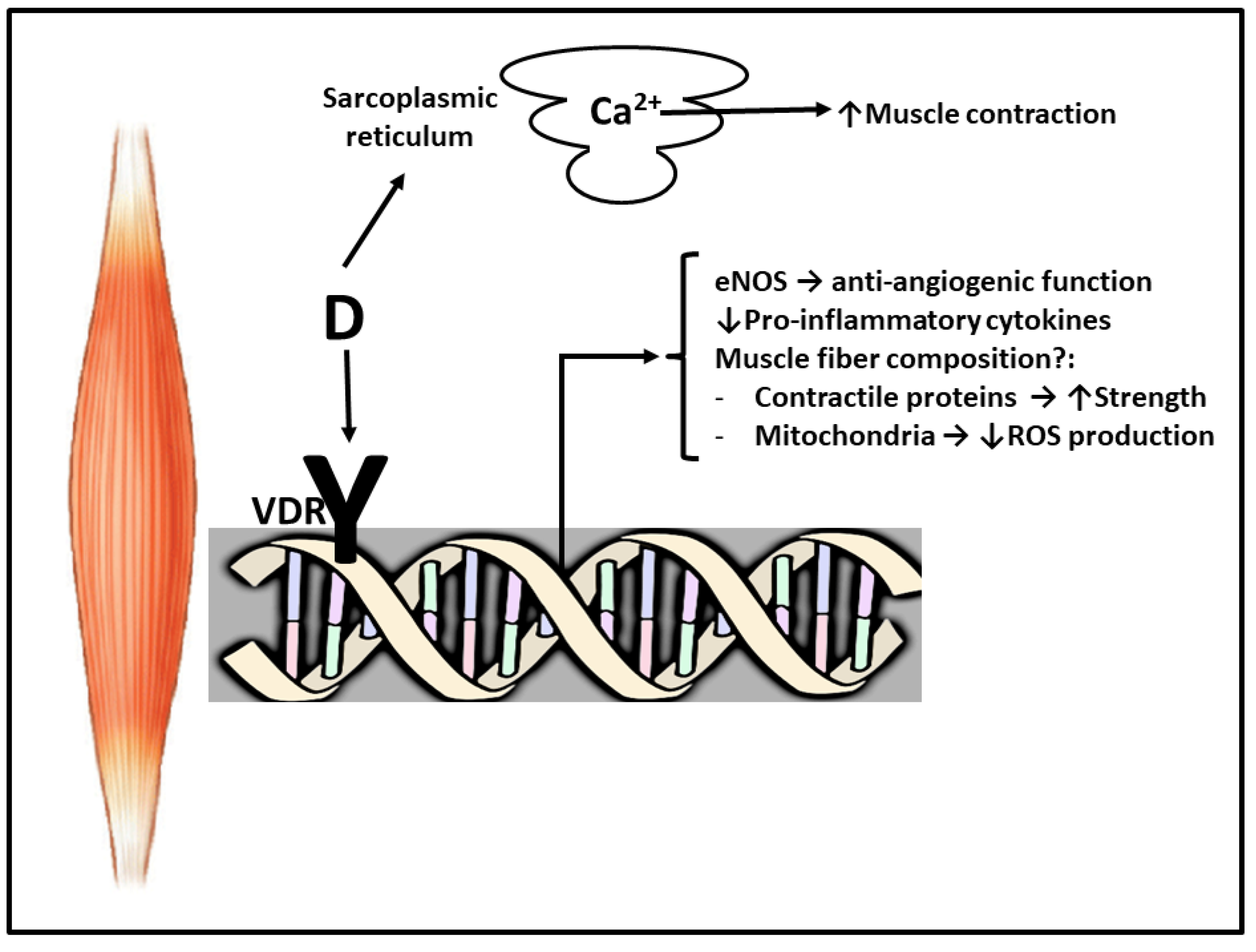
Vitamin D is commonly associated with calcium and bone health, yet its role in muscle is more orchestral than singular. It acts like a conductor for cellular rhythms—interacting with receptors present in muscle tissue and influencing processes tied to contraction, inflammation regulation, and mitochondrial function. When vitamin D status is low, muscles may lose some of their efficiency and recovery capacity. The result can be a subtle decline in strength, endurance, and even balance.
Imagine vitamin D as the luminescent thread in a tapestry. Without enough of it, the pattern still exists, but the weaving tightens in the wrong places. Strength becomes harder to sustain, and workouts can feel like they “cost” more. Over time, if the body also experiences reduced intake from a weight-loss trajectory, the risk of muscle loss may rise.
Vitamin D also interacts with the inflammatory milieu. Chronic low-grade inflammation is like fog over a road: you can still travel, but you can’t see potholes early. Muscle tissue is sensitive to these signals; inadequate vitamin D may leave recovery systems working slower, which can impair the body’s ability to adapt to training.
The coupling: how vitamin D status may amplify muscle vulnerability during semaglutide treatment
The link is rarely linear, and that’s precisely what makes it compelling. Semaglutide can encourage weight reduction, which can lower muscle mass if protein intake, training, and micronutrient status don’t counterbalance the shift. Vitamin D status may act as an amplifier in that scenario—either dampening decline or, when deficient, making muscle harder to preserve.
Consider a ship traveling through two conditions: fewer provisions and rougher seas. Semaglutide can be viewed as part of the provisions adjustment. Vitamin D adequacy can be viewed as the condition of the ship’s hull integrity. If the hull is sturdy, the ship navigates storms with less structural stress. If the hull is weak—due to deficiency—the same voyage can lead to more wear.
When vitamin D is sufficient, the body may be better equipped to support protein utilization, repair muscle microdamage from exercise, and maintain neuromuscular coordination. When vitamin D is insufficient, the “repair crew” can be delayed, and the body may rely more on muscle tissue to meet energy demands during sustained calorie reduction.
Not every person experiences the same outcomes. Genetics, baseline fitness, dietary composition, sun exposure, age, and concurrent comorbidities all modify the picture. Yet the logic remains: when muscle is asked to do more with less, the biochemical environment matters.
Why weight loss strategies often need a muscle-first redesign
Many weight-loss approaches inadvertently become muscle-loss strategies by omission. Calorie reduction is only half the equation. Protein adequacy, resistance training, and micronutrient sufficiency complete the triad. Without that triad, muscle becomes the “easy target.”
A muscle-first redesign turns the narrative from “How fast can weight drop?” to “How well can muscle stay functional while weight declines?” This is where vitamin D enters the scene as a supportive infrastructure rather than a standalone solution.
In practical terms, muscle-friendly weight loss tends to include: consistent strength training; adequate protein distribution across the day; and attention to vitamin D status—especially in individuals with limited sun exposure, darker skin, older age, malabsorption risk, or prior vitamin D insufficiency.
Intriguing visuals: vitamin D’s muscle action and the “energy-to-strength” bridge
Some concepts become easier to grasp when your mind can “see” them. Vitamin D is often depicted as moving through pathways that influence muscle function and responsiveness. These diagrams highlight how vitamin D action is not merely about bones—it reaches into muscle signaling, cellular regulation, and functional performance.

In another visual framing, vitamin D is linked to mechanisms supporting muscle growth and functional capacity. When you combine these ideas with the body’s need to maintain strength during weight loss, vitamin D becomes less like a passive nutrient and more like an active mediator.
Potential risk patterns: who should be extra alert
Muscle loss risk is not evenly distributed. Several patterns may elevate vulnerability during semaglutide-associated weight reduction. Older adults are at higher baseline risk due to sarcopenia trends—an age-linked drift toward lower muscle mass and strength. People with low baseline vitamin D levels may experience greater muscular effects if deficiency is not addressed. Those who reduce activity during weight loss can also lose muscle faster, because training stimulus is part of the maintenance system.
Additionally, individuals with low protein intake, limited access to resistance training, or inadequate dietary quality may face a convergence of risks. The most precarious scenario resembles a tightening knot: reduced calories, inadequate protein, decreased training stimulus, and low vitamin D status. Unraveling just one strand can help. Unraveling more can transform outcomes.
Safeguarding muscle: practical strategies that harmonize semaglutide, vitamin D, and training
Muscle protection is best approached like a layered defense. Begin with strength training—progressive overload if possible. Then aim for protein adequacy and distribute it across meals. Finally, treat vitamin D status as a measurable variable rather than a vague assumption.
Vitamin D optimization usually involves checking serum 25(OH)D levels and following a clinician-guided plan for supplementation if needed. Timing matters too: many people align supplementation with consistency—taking it regularly rather than sporadically. Sun exposure can contribute, but it varies widely by geography, season, skin coverage, and individual considerations.
There is also an underappreciated behavioral lever: recovery. Sleep quality affects hormonal signaling and muscle repair. If sleep deteriorates during weight loss, muscle preservation becomes even more difficult.
When the conversation turns: symptoms, monitoring, and actionable follow-through
Muscle loss can show up as more than scale changes. Consider subtle signs: reduced strength on familiar tasks, slower recovery after workouts, increased fatigue, or a decline in balance and coordination. If weight loss progresses while strength declines, that mismatch deserves attention.
Monitoring can include objective measures such as tracking strength performance, considering body composition assessments when available, and reviewing lab markers related to vitamin D status when clinically indicated. The goal isn’t alarm—it’s clarity. Clarity enables early adjustments: protein refinement, training recalibration, and vitamin D optimization.
The unique appeal: a “composed” approach to body transformation
The most compelling approach to semaglutide and muscle loss isn’t panic-driven. It is composed. It treats weight loss as a choreography, not a demolition. Vitamin D contributes to this choreography by supporting neuromuscular function, cellular regulation, and recovery capacity—especially during periods when the body is under nutritional pressure.
Put simply: semaglutide may tilt the stage, but vitamin D can help strengthen the footing. With strength training as the choreography and nutrition as the rhythm, muscle becomes less of a casualty and more of a collaborator. The transformation becomes not just smaller, but sturdier—an outcome that feels powerful, not merely achieved.
Conclusion: building resilience at the intersection of semaglutide and vitamin D
The link between semaglutide, vitamin D, and muscle loss is best understood as an intersection of forces: energy balance, training stimulus, protein adequacy, and micronutrient signaling. Vitamin D can serve as a stabilizing influence, potentially helping the body maintain muscle performance while weight decreases. But muscle-first strategy is still essential. The body does not preserve itself by hope alone; it preserves itself through consistent inputs.
For anyone using semaglutide, the most intriguing question isn’t only “Will I lose weight?” It’s also: “Will I keep my strength?” And that question is where vitamin D, thoughtfully managed, can become a meaningful ally.





