When the bloodstream becomes a crowded avenue, every molecule is a passenger with an agenda. Warfarin is the conductor—carefully lowering the odds of a clot forming—while “high-dose D” (vitamin D at elevated intake) can act like unexpected weather: not always dramatic, but capable of shifting traffic patterns in subtle ways. The intrigue lies in the overlap between coagulation chemistry, vascular biology, and vitamin-mediated signaling. Some people hope that more vitamin D means more safety; biology, however, prefers nuance. Understanding the interaction of high-dose vitamin D with warfarin is less about fear and more about reading the fine print of human physiology.
Warfarin and Vitamin D: Two Systems, One River
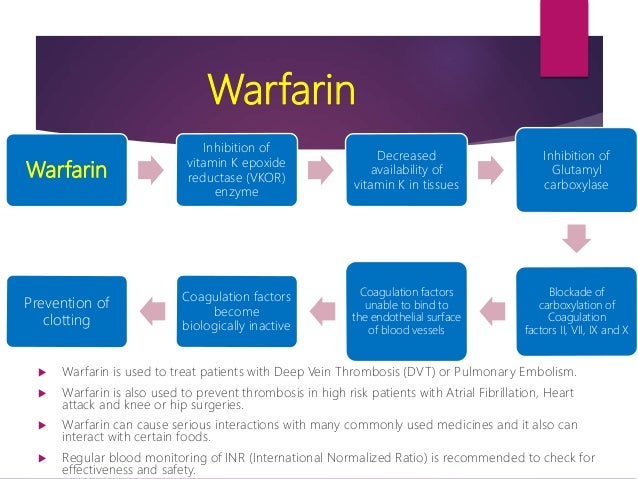
Warfarin’s central mission is to interfere with vitamin K–dependent clotting factors. It does not simply “thin” blood like a uniform veil. Instead, it reshapes the production landscape of proteins that stabilize a clot’s scaffolding. Think of vitamin K as the ink for clotting-factor blueprints; warfarin asks the cell’s printing press to miss key steps.
Vitamin D, by contrast, is less a direct clotting agent and more a molecular translator. It influences gene expression through the vitamin D receptor, affecting calcium balance, immune behavior, endothelial function, and inflammatory signaling. In normal doses, vitamin D supports skeletal integrity and modulates multiple pathways that touch cardiovascular health.
When vitamin D dosing becomes “high,” the conversation changes. The body can tip from compensatory adaptation into dysregulation—where mineral homeostasis and signaling become overstimulated. The possible interaction with warfarin is therefore indirect but consequential: altered physiology can nudge the INR trajectory, affect dosing stability, or amplify risks that intersect with anticoagulation management.
Defining “High-Dose D” and Why Dose Shape Matters
High-dose vitamin D isn’t one single number; it’s a category of intake that elevates blood 25-hydroxyvitamin D well above typical targets. What matters most is dose magnitude and duration, alongside baseline vitamin D status, kidney function, dietary calcium, and concurrent supplements.
A small excess may be metabolically tolerated, like extra rain in a reservoir. But sustained, high intake can raise the possibility of vitamin D–mediated hypercalcemia—an imbalance that can influence vascular behavior and overall stability.
Warfarin therapy is famously sensitive to “small” physiological disturbances. INR is a barometer that reacts not only to medications, but also to shifts in diet, liver metabolism, illness, and absorption patterns. High-dose vitamin D can therefore become part of the background noise that turns into measurable signal.
The Indirect Bridge: Inflammation, Endothelium, and Coagulation Crosstalk
Coagulation does not live in isolation. The endothelium—the inner lining of blood vessels—sends pro- and anti-thrombotic instructions. Vitamin D influences inflammatory mediators and immune signaling, which can indirectly affect endothelial tone.
Warfarin aims at clotting-factor availability, but thrombotic tendency also reflects the vessel wall’s mood. In a less inflamed environment, the tendency to form clots may be reduced; in an inflamed environment, the coagulation system can become more reactive. High-dose vitamin D may, depending on context, push immune signaling in ways that influence this delicate balance.
Even when vitamin D does not directly alter warfarin’s pharmacologic target, it can alter the terrain on which warfarin operates—like changing the ground beneath the same bridge.
INR Stability: Where Patients Feel the Difference
Patients on warfarin often describe the experience in a concrete way: “My INR is more jumpy” or “My dose feels unpredictable.” Those observations matter. INR stability depends on steady metabolism and consistent clotting-factor turnover.
High-dose vitamin D may contribute to variability through several routes: changes in calcium and parathyroid signaling, possible effects on liver enzyme activity in certain contexts, and the broader metabolic state of the patient. Not every patient will experience a change, but the possibility justifies careful monitoring.
INR is not merely a number; it’s a surveillance language. When vitamin D intake escalates, clinicians may consider closer INR checks to ensure the therapeutic window remains intact.
Hypercalcemia Risk: When Chemistry Becomes a Domino Chain
One of the more dramatic consequences of high-dose vitamin D is hypercalcemia or elevated calcium-related indices. Calcium is not just for bones; it plays roles in vascular smooth muscle behavior, cellular signaling, and coagulation-adjacent cellular processes.
If vitamin D intake pushes calcium too high, the body can respond with nausea, constipation, fatigue, confusion, dehydration, and renal stress. Kidney impairment can then complicate warfarin management indirectly—affecting overall metabolism, medication tolerance, and physiologic stability.
The danger is less that vitamin D “directly cancels warfarin” and more that it sets off a chain reaction that makes anticoagulation management harder to keep steady.
Vitamin K, the Missing Note in the Symphony
Warfarin’s dependence on vitamin K means dietary patterns are powerful. Vitamin D and vitamin K often travel together in nutrition discussions because both relate to cardiovascular and skeletal health. Yet vitamin K intake can fluctuate with foods and supplements, and these variations can dominate the clinical picture.
High-dose vitamin D might be taken alongside changes in diet—such as increased dairy consumption, fortified foods, or added supplements marketed for “bone support.” If those changes also include vitamin K, INR could shift. Conversely, if someone takes vitamin D heavily but simultaneously reduces vitamin K foods, anticoagulation sensitivity could increase.
In practice, the interaction is often a triangulation: warfarin + vitamin D + vitamin K patterns. The “metaphorical clock” moves differently depending on which hands are adjusted.
Food Supplements and Absorption: The Real-World Variables
Supplement formulation matters. Some vitamin D products are fat-soluble, and absorption can vary with meal composition, gastrointestinal health, and adherence. A person who begins taking vitamin D with a higher-fat meal may experience a faster rise in vitamin D levels than someone who takes it on an empty stomach.
Warfarin absorption and metabolism can also be influenced by other factors: inconsistent dosing habits, interacting medications, alcohol intake, and liver health. When these variables stack, it can appear as though vitamin D alone is responsible.
But biology rarely acts solo. Instead, it behaves like a layered playlist—each track changing the overall sound.
Medication Interactions: The Wider Network Around Warfarin
Warfarin interacts with many drug classes: some medications accelerate clearance, others inhibit metabolism, and some alter vitamin K availability. Vitamin D may not be among the most famous direct culprits, but high-dose supplementation can still coincide with other changes—multivitamins, omega-3 preparations, magnesium/calc combinations, or steroid regimens.
Even lifestyle changes—sun exposure, dietary alterations, weight changes—can alter the body’s metabolic balance. When high-dose vitamin D is introduced in a patient already under anticoagulation management, it’s wise to consider the entire ecosystem of substances, not only the one supplement.
Monitoring and Safety: Keeping the Therapeutic Window Bright
If high-dose vitamin D is considered while taking warfarin, monitoring becomes an anchor. That typically means checking INR more frequently during the initiation period and after dose adjustments. Symptoms should also be treated as clues rather than inconveniences—especially any signs of bleeding.
Bleeding red flags include unusual bruising, prolonged bleeding from cuts, nosebleeds, blood in urine or stool, black tarry stools, severe headache, dizziness, or weakness. These aren’t “wait and see” events; they’re stop-and-assess signals.
Safety is not a mood; it’s a system. In that system, communication between patient and clinician is as critical as the lab results.
Choosing a Sensible Strategy: Precision Over Extremes
The unique appeal of understanding this interaction is empowerment. It allows decisions to be made with clarity rather than instinct. Instead of treating vitamin D as a simple “more is better” lever, the wiser approach is calibration—measuring blood levels, accounting for baseline deficiency, and avoiding unnecessary escalation.
Warfarin therapy thrives on steadiness. Vitamin D can be supportive, but high-dose regimens should be purposeful, supervised, and monitored. The goal is a calm therapeutic landscape: appropriate vitamin D status without destabilizing anticoagulation control.
Looking Ahead: The Metaphor of Balance
Imagine warfarin as a lighthouse beam in a storm—guiding clotting-factor activity into a safer lane. High-dose vitamin D is the shifting tide outside the harbor: not always visible, but capable of influencing what the vessel must do to stay on course. The interaction may be indirect, yet it is real in the lived experience of INR variability, physiological stress, and dietary dynamics.
When high-dose vitamin D enters the warfarin story, the best practice is neither alarmist nor complacent. It’s attentive, evidence-informed, and measured. In the bloodstream’s ever-moving theater, precision is the quiet hero.