
For years, vitamin D has occupied a curious niche in everyday health: part nutrient, part hormone-like messenger, part quiet guardian of bone and muscle. Then a different story sometimes surfaces—one told in case reports, where “high-dose” vitamin D appears to cast a longer shadow than expected. The phrase “kidney failure” does not belong in the same sentence as vitamin D in most people’s minds. Yet, in clinical narratives, it occasionally does. What begins as supplementation intended to correct a deficiency can—under certain circumstances—become a detour toward hypercalcemia, renal stress, and, in severe instances, irreversible decline. The pattern is unsettling, but it is also deeply instructive, because it hints at how fragile biology can be when a system is nudged too far in the wrong direction.
Why “High-Dose” Changes the Conversation
Most discussions about vitamin D emphasize benefits: improved calcium absorption, better skeletal integrity, perhaps even modulation of immune function. But “high-dose” is not merely a larger amount—it is a different physiological tempo. Vitamin D’s active metabolites can raise serum calcium and influence phosphate balance. In turn, calcium can alter kidney physiology, particularly when concentrations climb rapidly or linger at high levels.
Case reports often share a common observation: an individual who took vitamin D at doses higher than routine replacement later presented with worsening kidney function. The timeline can be striking. Symptoms may start subtly—nausea, fatigue, constipation—but quickly progress. The kidney, which normally filters waste and regulates mineral equilibrium, becomes collateral damage when calcium overload begins to dominate.

It is worth noting the irony: vitamin D is often chosen to protect health, yet the same compound—when overdosed—can provoke the very organ stress it was meant to support. This contradiction is part of the fascination. It suggests that supplementation is not a universal remedy; it is an intervention with boundaries.
Hypercalcemia: The Usual Culprit Behind Renal Decline
When vitamin D dosing overshoots, hypercalcemia becomes the main plot mechanism in many cases. Elevated serum calcium can lead to dehydration through effects on renal concentrating ability, and it can trigger renal vasoconstriction. The body may respond with thirst and frequent urination at first. Later, a vicious cycle can emerge: volume depletion plus mineral toxicity means the kidney experiences a double hit—less perfusion and more biochemical injury.
Beyond dehydration, high calcium levels can promote nephrocalcinosis. Calcium may deposit in renal tissue, forming microcrystals that interfere with tubular function. This is not a dramatic explosion; it is a gradual erosion of function, often expressed as rising creatinine, reduced urine output, and electrolyte abnormalities.
Some reports describe patients who were not profoundly ill at the outset. They had the calm, ordinary context of supplementation. Then laboratory results revealed a biochemical storm—calcium values climbing well above normal, sometimes accompanied by suppressed parathyroid hormone (depending on the scenario), and deteriorating renal indices.
How Renal Physiology Turns Fragile Under Mineral Overload
To understand why kidneys can fail in these cases, it helps to picture the kidney as a precision filtration-and-regulation organ. The nephrons are not passive pipes. They actively adjust to mineral gradients, maintain acid-base balance, and reabsorb key ions.
High calcium disrupts these finely tuned processes. Tubular cells can become stressed, and the normal handling of calcium and other electrolytes may falter. When calcium is excessive, it can interfere with sodium reabsorption, alter urine composition, and increase the likelihood of crystalline obstruction. The result is often acute kidney injury—sometimes severe—though chronic progression is possible if the toxic exposure persists.
The fascination here lies in the specificity: vitamin D itself might not “directly” destroy kidney tissue in the way some nephrotoxic agents do. Instead, vitamin D’s downstream mineral effects can reorganize kidney function into a less sustainable state. In other words, the kidney fails because the environment becomes inhospitable.
The Patterns Seen in Case Reports
Case reports, by their nature, are not statistical maps. Still, they often converge on similar themes.
First, there is frequently a mismatch between dose and monitoring. Some patients take vitamin D daily or in bolus forms, sometimes without frequent checks of serum 25-hydroxyvitamin D and calcium. The system then drifts. Blood levels can rise silently until they cross a threshold where symptoms begin and renal parameters worsen.
Second, comorbidities appear often. Underlying chronic kidney disease, disorders that predispose to hypercalcemia, granulomatous diseases, and conditions associated with increased calcium absorption can amplify risk. A person may tolerate moderate supplementation, but not tolerate a specific combination of dose, physiology, and medical background.
Third, the medication landscape can contribute. Concomitant agents that affect calcium or kidney perfusion—directly or indirectly—can create an additive hazard. Even lifestyle and hydration status matter. A patient with limited fluid intake may experience faster dehydration when calcium rises.
Who Might Be More Vulnerable—and Why
Not everyone experiences renal catastrophe from high-dose vitamin D. Susceptibility tends to cluster around biological context.
Individuals with baseline reduced renal reserve are less able to buffer mineral excess. If the kidneys already operate at the edge of function, even modest deviations can be consequential. Meanwhile, conditions such as primary hyperparathyroidism can shift calcium regulation toward higher set points, making vitamin D’s effect more pronounced.
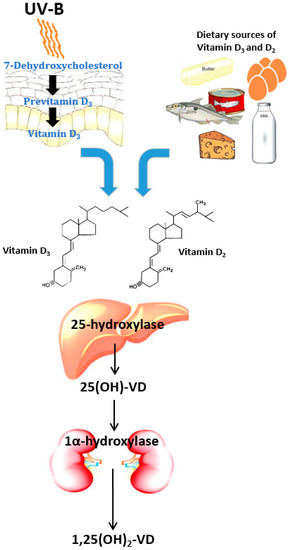
Another layer involves the conversion of vitamin D to active forms. Some patients may have altered metabolic processing—whether due to disease states, organ function variability, or genetic differences in vitamin D binding proteins. The result is that two people taking the “same” dose may generate different blood-level dynamics.
As the body’s feedback loops tighten around calcium balance, the kidney becomes a vulnerable final interpreter. This is why risk is not solely about dosage; it’s also about timing, individual biology, and the presence of hidden accelerants.
The Role of Dosing Strategies, Including Bolus Therapy
High-dose regimens are not all alike. Daily dosing, weekly dosing, and occasional bolus administration can produce different peaks and troughs in serum vitamin D metabolites. Peaks can matter: a transient surge of active metabolites may push calcium above a critical point before the system can compensate.
In some narratives, vitamin D was prescribed to correct a deficiency or to “reach a target quickly.” Yet rapid correction can reduce the margin for error if laboratory monitoring is delayed. The kidney can’t wait for ideal timing; it responds in real time to biochemical conditions.
Even a well-intentioned strategy can become precarious when adherence is unclear, when other supplements add to the total intake, or when the original deficiency was not fully characterized. A fascinating aspect of these reports is how they sometimes reveal a hidden cumulative arithmetic—multiple sources of vitamin D, plus dietary supplements, plus fortified products, all stacking into an unintended high-dose reality.
Symptoms That Often Appear Before Kidney Failure
In the earliest phase, symptoms may be vague. Fatigue can arrive like a fog. Gastrointestinal disturbances may follow—nausea, vomiting, abdominal discomfort, constipation. Confusion and muscle weakness may emerge if calcium becomes markedly elevated.
These signs are not unique to vitamin D toxicity. That’s why clinical vigilance matters. A patient with persistent gastrointestinal symptoms after starting or increasing vitamin D might not immediately trigger suspicion of hypercalcemia in every setting. Case reports suggest that when these symptoms are paired with abnormal labs—high calcium, elevated creatinine, and signs of dehydration—the plot becomes legible.
Diagnosis: Connecting the Dots Clinically
Clinicians typically look for a constellation: elevated serum calcium, evidence of kidney injury, elevated vitamin D metabolites in many cases, and exclusion of alternative causes such as other nephrotoxic exposures. Urinalysis may show changes consistent with mineral stress. Imaging sometimes helps identify nephrocalcinosis if deposits have formed.
Importantly, diagnosis is not merely labeling vitamin D as the villain. It is understanding mechanism. If hypercalcemia drives the renal decline, then the management pathway changes: calcium must be reduced, hydration supported, and vitamin D exposure halted. The narrative logic matters because it predicts recovery potential—and recovery is not guaranteed.
Treatment and Recovery: What Usually Happens Next
When vitamin D toxicity is suspected, treatment tends to prioritize immediate stabilization. Stopping supplementation is the first decisive step. Hydration supports renal perfusion and helps clear excess calcium. Sometimes clinicians use medications that reduce calcium reabsorption or lower serum calcium through specific metabolic pathways.
As calcium normalizes, kidney function may improve—sometimes dramatically. Yet some reports describe incomplete recovery, especially when exposure was prolonged or when deposits had already formed. This introduces a sober lesson: the kidney can recover, but there is a window. Waiting too long risks making a biochemical issue into structural damage.
There is also a long-tail dimension. After the acute episode, patients may need a cautious reintroduction of vitamin D—if reintroduction is even appropriate—along with structured monitoring plans.
Practical Lessons: Monitoring, Dose Limits, and Mindful Use
The overarching message from case reports is not that vitamin D is universally dangerous. It is that vitamin D is powerful enough to be risky when administered without individualized calibration and follow-up.
Monitoring is the fulcrum. Measuring 25-hydroxyvitamin D can confirm whether deficiency truly exists and whether replacement is working. Serum calcium helps ensure the body is not moving into hypercalcemic territory. For individuals at higher risk—those with kidney impairment or other predisposing conditions—monitoring should be more frequent and thresholds should be taken seriously.
Equally important is dose arithmetic. “High-dose” should be contextualized: combined supplements, fortified foods, and multiple vitamin products can inflate total vitamin D intake without the patient realizing it. Education isn’t an afterthought; it is part of safety engineering.
Deeper Reasons for the Ongoing Fascination
Why do these narratives continue to intrigue clinicians and readers alike? Because they sit at the intersection of reassurance and warning. Vitamin D is often framed as a benign wellness supplement, almost like an optional insurance policy. Yet kidney failure stories remind us that the body’s safety margins are not infinite.
These case reports reveal the choreography of human physiology: how biochemical peaks can outpace regulatory systems, how dehydration and mineral stress can converge, and how the kidney—so often imagined as durable—can falter under mineral imbalance. They also show the importance of time: the interval between dose increase and lab monitoring can determine whether the episode resolves smoothly or leaves lasting injury.
In the end, the link between high-dose vitamin D and kidney failure is less about vitamin D as a single substance and more about the complex ecosystem it inhabits. When dose, metabolism, hydration, comorbidity, and monitoring collide unfavorably, the kidney becomes the messenger that delivers the warning. The lesson is not fear. It is precision.




