
Ever wondered whether your heart cares about the alphabet on your vitamin bottle? D2 or D3—two names, one mission, and potentially different cardio-reverberations. Now here’s the playful question: if your bloodstream were a busy city, would ergocalciferol (D2) be a dependable delivery van, or would cholecalciferol (D3) arrive like an express helicopter? Before you decide, prepare for a small challenge—because the “best” form isn’t just a label. It’s a chain of biochemical choreography, absorption quirks, and how your body behaves when cardiovascular risk is on the horizon.
D2 vs D3: the quick origin story (and why it matters for the heart)
Vitamin D comes in multiple forms, but D2 and D3 are the headline stars. D2 is commonly called ergocalciferol, traditionally associated with plant-derived sources and certain supplements. D3 is cholecalciferol, often linked with sunlight exposure and animal-based sources, though supplements exist in both forms.
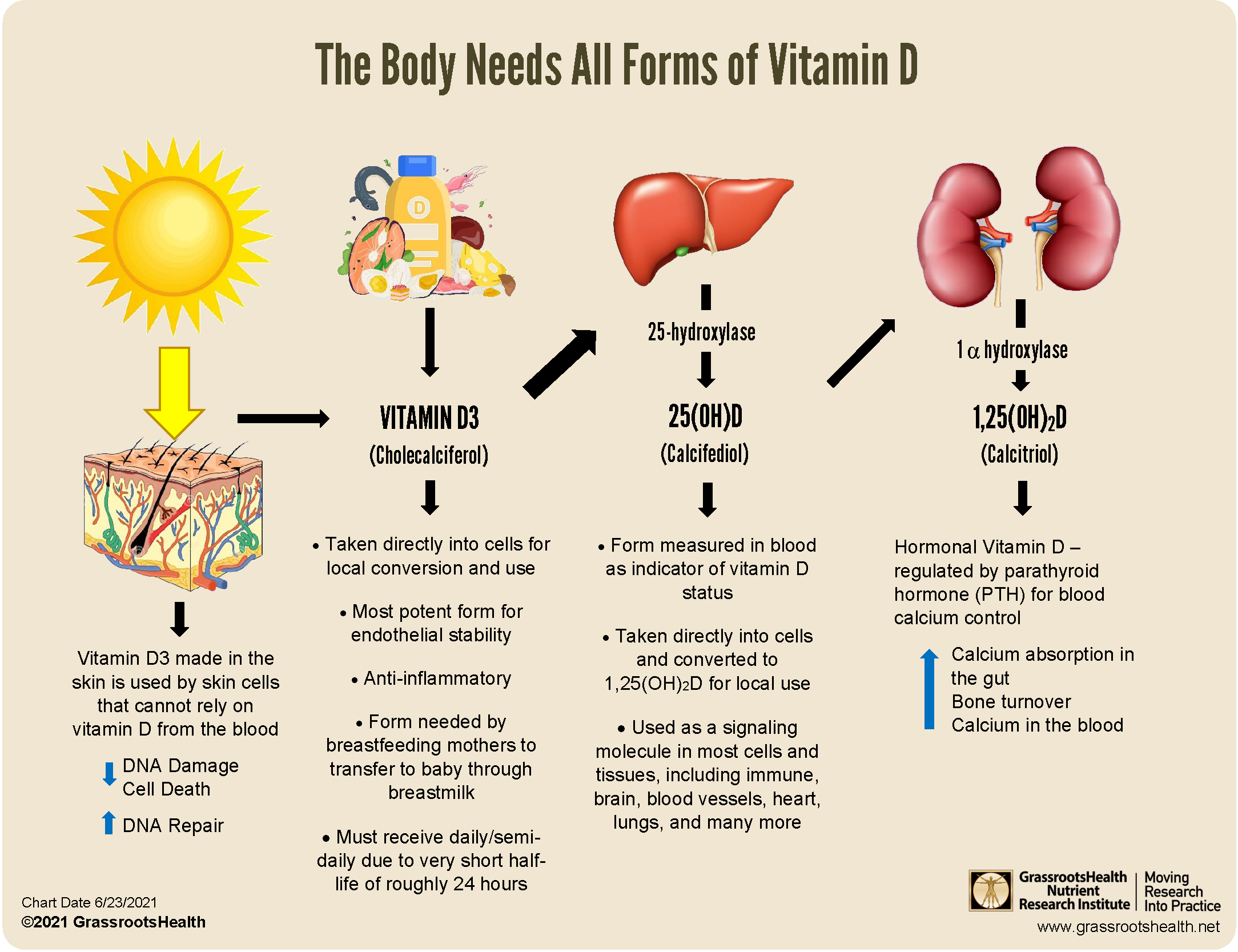
Why should the heart care? Because vitamin D isn’t merely about bones and sunshine nostalgia. It becomes active through conversion steps in the liver and kidneys, ultimately supporting processes that relate to vascular function, inflammation modulation, and cardiometabolic regulation. In other words, vitamin D acts less like a single nutrient and more like a signaling molecule with a broad civic role.
So the question becomes: which form turns into the outcomes your cardiovascular system prefers?

Bioavailability and potency: the “who raises the level better?” debate
One of the most practical comparisons between D2 and D3 involves their ability to raise and sustain blood levels of 25-hydroxyvitamin D—often abbreviated as 25(OH)D. This circulating form is considered a key marker of vitamin D status.
D3 tends to be favored in many real-world contexts because it often shows stronger potency for elevating 25(OH)D. That doesn’t automatically mean D2 is ineffective. It can still contribute, especially when dosing is appropriate and consistent. But heart health is not a one-and-done event; it’s cumulative, influenced by sustained biochemical conditions over time.
Imagine two gardeners watering a plant. One form delivers a steadier supply; the other might require a different watering schedule to achieve the same growth pattern. For the cardiovascular “garden,” stability can be a subtle advantage.
Conversion efficiency: the biochemical relay race
Vitamin D undergoes transformation—first from its supplement form to storage and transport stages, then onward toward active signaling forms. This is a relay race with checkpoints in the liver and kidneys. Small variations in how D2 and D3 are processed can influence the duration and intensity of downstream effects.
In everyday terms: if D2 and D3 produce different patterns of circulating vitamin D metabolites, the “signal” reaching vitamin D receptors may vary. Those receptors are present in tissues that matter for cardiovascular health, including vascular cells and components tied to immune response.
When inflammation is amplified or vascular responsiveness is impaired, the body benefits from regulatory inputs. Vitamin D’s signaling role can contribute to that regulation—though it’s not a magic wand.
Heart health mechanisms: what vitamin D may influence beyond cholesterol
Let’s zoom out to the heart’s neighborhood. Vitamin D is frequently discussed in relation to:
Inflammatory tone: Chronic low-grade inflammation can be a simmering backdrop for cardiovascular risk. Vitamin D may help nudge immune activity toward balance.
Vascular function: The endothelium—the vessel lining—controls dilation and blood flow. Vitamin D may support healthier vascular responsiveness.
Blood pressure regulation: Some research connections suggest associations between vitamin D status and blood pressure outcomes, though results vary by population and methodology.
Cardiometabolic interplay: Vitamin D is also linked with insulin sensitivity and broader metabolic pathways that can indirectly affect heart health.
Here’s the twist: these pathways don’t hinge on a single variable. They depend on overall status, baseline deficiency risk, lifestyle factors, and whether vitamin D levels are consistently maintained.
D2 or D3 for cardiovascular outcomes: how to think like a realist
When comparing D2 and D3 for heart health, it helps to avoid overly binary thinking. “Better” often means “more reliable under typical supplementation conditions.” D3 is commonly associated with more robust increases in 25(OH)D for many people, which may make it a practical choice when aiming to correct low vitamin D status.
However, D2 can still be reasonable, particularly when it’s available, tolerated, and dosed correctly. If someone starts with severe deficiency, adherence and dosing strategy become critical. Two people can take the same labeled dose and end up with different blood levels because absorption, body composition, and baseline status vary widely.
So the better question isn’t only “D3 or D2?” It’s “Which one will help you reach and maintain adequate 25(OH)D consistently?” That’s where heart health logic becomes clearer.
Dosing and consistency: the challenge you should not ignore
Now for the challenge—consider this: will you take vitamin D in a way that actually maintains levels through the seasons?
D3 and D2 may require different dosing schedules depending on potency and the specific product. Many clinicians emphasize regular intake because vitamin D is not a short-term supplement; it’s closer to a long-running broadcast that your body tunes into.
Also, vitamin D absorption improves when taken with dietary fat. A capsule with a bland, fat-free routine may underperform compared with the same capsule taken alongside a meal that includes some lipids.
If heart health is the goal, inconsistency can be the silent saboteur. A supplement that corrects deficiency today but fails to maintain levels next month is less supportive than a steady regimen.
Safety considerations: how to avoid the “too much of a good signal” problem
Vitamin D is fat-soluble, which means it can accumulate. That’s why upper limits and appropriate monitoring matter—especially for individuals with kidney disease, sarcoidosis, certain granulomatous disorders, or those taking medications that affect calcium metabolism.
Excess vitamin D can lead to hypercalcemia in susceptible individuals, which is not a heart-friendly direction. Symptoms can include nausea, constipation, excessive thirst, confusion, and in severe cases more serious complications.
The safest strategy is not guessing. It’s measuring baseline 25(OH)D, setting an evidence-informed target, and rechecking after a reasonable interval.
Which form should you choose? a practical decision pathway
Here’s a grounded way to decide between D2 and D3:
Start with your vitamin D status: If you’re deficient or low, choose the form that your dosing plan can reliably elevate and sustain.
Prioritize adherence: The “best” form is the one you actually take consistently, in a way that supports absorption.
Use monitoring as a compass: Recheck 25(OH)D and adjust, rather than relying on assumptions.
Consider your health context: Heart disease risk, kidney function, and medication profile can influence tolerability and dosing needs.
In many cardio-minded supplement plans, D3 is often selected because it is frequently associated with more reliable improvements in vitamin D levels. Yet the individualized plan remains the deciding factor, not the chemistry alone.
The bigger picture: vitamin D is a piece of the heart-health mosaic
Even if you pick the superior form, vitamin D won’t outrank foundational cardio strategies. Think of your heart as a mosaic, not a single tile. Nutrition patterns, physical activity, sleep quality, blood pressure control, smoking status, and lipid management are the larger structural beams.
Vitamin D may function like supportive lighting—helpful, sometimes transformative, but best viewed as part of an integrated environment. When vitamin D status improves, it can complement a broader approach to cardiovascular wellness.
Closing thought: your heart’s vote might depend on your levels, not the label
So—D3 or D2? If heart health were a courtroom, D3 often enters as the more consistently persuasive witness: commonly linked with stronger increases in 25(OH)D and the potential for steadier maintenance when taken appropriately. But the verdict should still consider your bloodwork, dosing rhythm, and overall health context.
Now the real challenge: don’t let vitamin D become an occasional cameo. Make it a planned, measurable part of your regimen. Your heart tends to thrive on consistency—especially when the chemistry is working in harmony.

