
You’ve probably heard the simple advice: “Get more vitamin D for stronger bones.” But the real question is more nuanced, almost tantalizingly so. Which form of vitamin D does the body actually prefer when the goal is better calcium absorption? The answer isn’t just a matter of chemistry—it’s a quiet story about conversion, timing, and the body’s own priorities. Let’s follow that story from the first pill to the moment calcium finally finds its way into bones.
Vitamin D Isn’t One Thing—It’s a Chain of Transformations
Vitamin D is often treated like a single nutrient, but it behaves more like a relay baton. Most people start with a precursor molecule, then the liver and kidneys perform selective “editing” to convert it into the active forms your body can use. That matters, because calcium absorption depends on the downstream, active outcome—yet the route you take to get there can influence how smoothly and reliably the final result happens.
There are two major dietary supplement “characters” in this relay: vitamin D2 (ergocalciferol) and vitamin D3 (cholecalciferol). Both can raise blood vitamin D levels, but they don’t always behave identically. Then there’s the more direct, medically-minded option: calcitriol, the active form that skips several conversion steps. Each option has a different tempo, a different “workflow,” and—sometimes—a different promise.
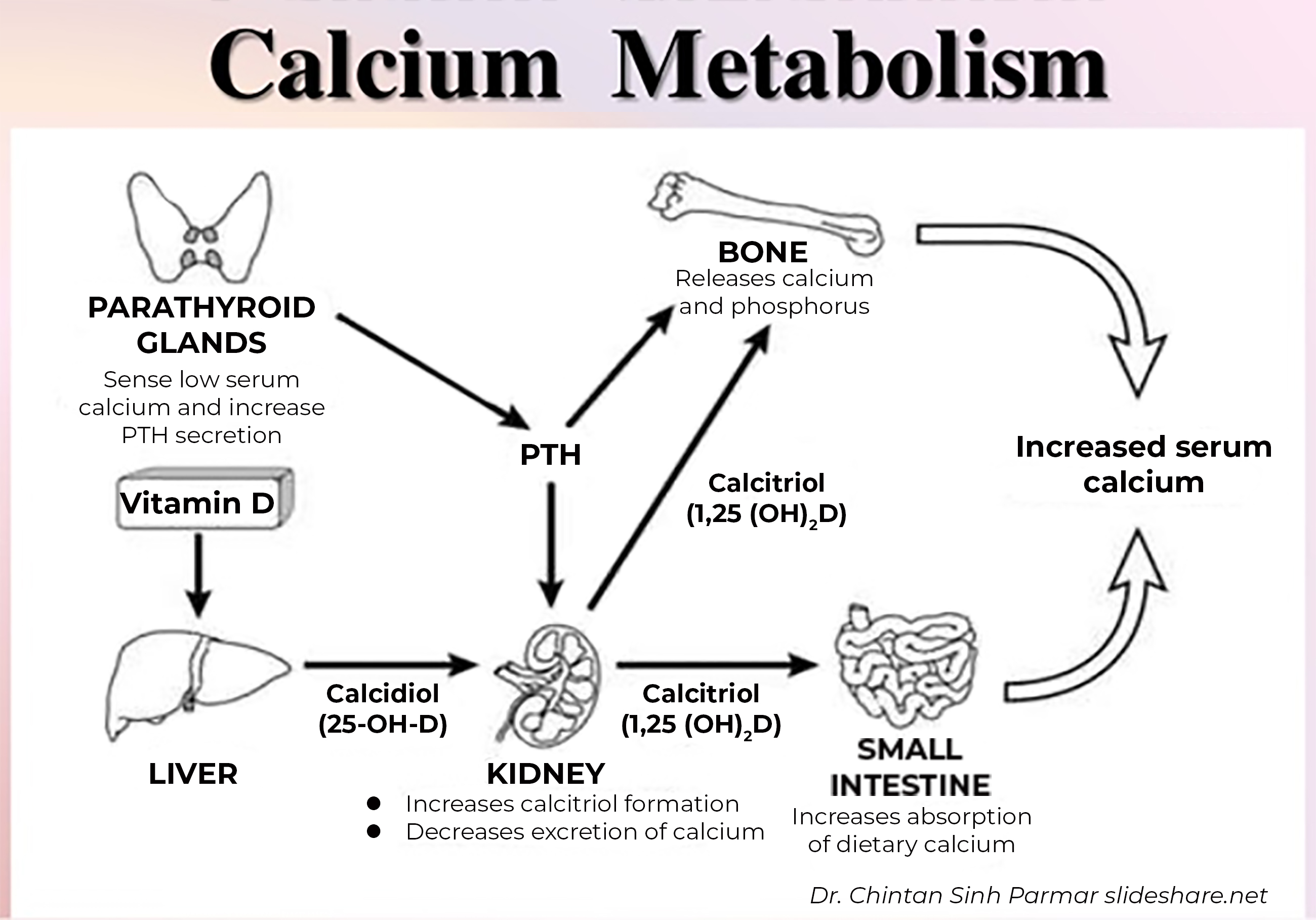
Here’s a useful visual to ground the concept that vitamin D and calcium metabolism are intertwined systems:
D2 vs D3: The Big Decision Most People Never Consider
When you see vitamin D on a label, it’s usually D2 or D3. D3 is the version produced in human skin after sun exposure. D2 is common in some plants and in certain fortified foods. Because D3 is closer to the body’s natural pathway, it can feel like the “home key.” But the more important question is whether it delivers a stronger downstream effect on calcium absorption.
Calcium absorption in the intestine is influenced by active vitamin D levels, which in turn support calcium-binding proteins and transport mechanisms. If D3 more effectively maintains or elevates those active levels, it can indirectly improve calcium absorption. Many individuals notice the difference not as a dramatic sensation, but as steadier progress over time—less wobble in lab values, better overall bone-support signals, and sometimes fewer “false starts” in repletion strategies.
Still, the comparison isn’t purely emotional; it’s mechanistic. Differences in molecular structure and in how each form is metabolized can affect how long vitamin D stays available in the body. Longevity of the “reserve” can be the hinge on which calcium absorption swings, particularly when dietary calcium is borderline or when daylight exposure is inconsistent.
How Calcium Absorption Actually Happens (And Where Vitamin D Fits In)
Calcium absorption isn’t a passive process. It’s coordinated, selective, and partly saturable. Vitamin D essentially acts as a transcriptional conductor: it increases the intestinal machinery that pulls calcium across the epithelial barrier. Without adequate vitamin D signaling, even generous calcium intake can be underutilized, like water pouring into a leaky reservoir.
There are two broad absorption pathways—active transport and passive diffusion. Active transport is the one vitamin D most strongly influences. When vitamin D status improves, the body tends to shift more calcium through that active, efficient route. This is why vitamin D deficiency can coexist with normal calcium intake yet still result in poor mineral handling.
Consider this a subtle invitation to shift perspective: vitamin D doesn’t merely “provide calcium.” It upgrades calcium’s capacity to be absorbed.
Which Form Is Typically Best for Absorption: D3 Often Wins the Conversation
For most people aiming to support calcium absorption through supplementation, vitamin D3 is frequently the preferred option. The reasoning often boils down to bioavailability and the ability to sustain vitamin D levels more effectively. If your goal is a consistent improvement in the body’s active vitamin D signaling, D3 tends to be a logical choice.
But “better” doesn’t mean “perfect for everyone.” Some individuals have unique circumstances—absorption disorders, kidney issues, malabsorption syndromes, or medication interactions—that can alter the timeline and success rate of conversion from precursor forms. In those cases, even a good form may not reach the active form with the same efficiency.
If you’re choosing between D2 and D3 for bone-oriented goals, it can help to ask not only “Which one raises vitamin D?” but also “Which one best supports the calcium-absorption pathway you care about?” That second question is where D3 often earns its reputation.
Calcitriol: The Shortcut Form—and Why It Isn’t for Everyone
Calcitriol is active vitamin D, meaning it can directly stimulate calcium absorption without waiting for the liver and kidney to complete earlier steps. This “shortcut” can be life-changing in specific clinical settings—particularly when conversion is impaired.
Yet calcitriol requires caution. Because it is already in the active form, it can increase calcium levels more rapidly and more directly than D2 or D3. For that reason, calcitriol is typically used under medical supervision, often when someone has certain kidney-related conditions or disorders of vitamin D metabolism. It’s powerful, but power demands precision.
So the curious twist is this: the form that is most effective in a mechanistic sense may not be the safest self-directed choice. The best form is often the one that fits your physiology, not just the one that sounds strongest.
Timing, Dose, and Consistency: The Hidden Variables
Even with the right form, absorption and outcomes depend on timing and dose. Vitamin D behaves like a slow-building reserve. Consistency matters. If you take vitamin D sporadically—especially large doses that leave long gaps—your body may fluctuate between “better signaling” and “not enough signaling.” Those swings can subtly affect calcium handling.
Also consider co-factors. Calcium absorption is influenced by dietary calcium, magnesium status, and overall gut health. A person with excellent vitamin D status but insufficient calcium intake may still struggle to reach the calcium targets that bones require.
Some people do better with doses split across days to reduce peaks and troughs. Others do well with weekly or monthly regimens. The optimal schedule depends on your body’s pattern of uptake and metabolism.
Sunlight, Skin Tone, and Real-Life Constraints
Natural sunlight produces vitamin D3. If someone lives in low-sun regions, works indoors, or has skin that generates vitamin D more slowly, vitamin D status can remain chronically low. In those scenarios, supplementation becomes less of a “nice-to-have” and more of a correction to a systemic gap.
But don’t forget that sunlight exposure also has trade-offs. Long-term sun avoidance can protect skin health while leaving vitamin D under-addressed. Supplement choice then becomes a practical bridge between two competing priorities: safeguarding skin and maintaining calcium absorption support.
Who Might Need a Different Approach?
People with malabsorption (such as celiac disease, inflammatory bowel conditions, or history of bariatric surgery) may not absorb vitamin D supplements efficiently. In these cases, the issue might not be D2 vs D3 at all—it might be delivery. Someone could take the “best” form and still struggle if absorption is impaired.
Similarly, kidney disease can reduce conversion to the active form. The body may have enough vitamin D substrate but lack the capacity to activate it. That is where calcitriol may enter the picture clinically.
Even medication can matter. Some drugs alter vitamin D metabolism. These scenarios are reminders that the “best” form depends on where the process breaks down in your specific pathway.
Testing and Tracking: The Only Way Curiosity Becomes Clarity
If you want to know which form is actually working for you, laboratory monitoring provides the missing chapter. Checking vitamin D status (typically 25-hydroxyvitamin D) can show whether supplementation is raising levels as intended. If calcium or related markers are abnormal, deeper investigation may reveal whether calcium absorption is truly improving.
Think of it as a feedback loop. Your body’s response can reveal whether you need a different form, a different dose, or a different therapeutic strategy altogether. Curiosity is useful—but measurement is what turns curiosity into certainty.
The Bottom Line: Choose the Form That Matches Your Physiology
For most people seeking better calcium absorption through supplementation, vitamin D3 is commonly the frontrunner. It aligns with human physiology and often supports a steady rise in vitamin D status that favors active signaling needed for intestinal calcium transport. D2 can help some individuals, but D3 typically offers a more reliable profile for maintaining vitamin D levels.
Calcitriol is the precision tool—remarkably effective when conversion is compromised, but typically not a DIY option due to its potency and the risk of calcium overshoot.
Ultimately, the best form isn’t just about chemistry. It’s about compatibility: your gut, your kidneys, your baseline vitamin D status, and your consistency. When those elements align, calcium absorption stops being a hope and becomes a practiced, dependable outcome.





