
Walk into any pharmacy aisle and you’ll notice how quickly “Vitamin D” becomes a single, simplified story. Yet for women thinking about osteoporosis prevention, the plot is richer than the label on the bottle. One detail—whether you’re getting D3 or D2—often gets treated like a footnote. It isn’t. Consider how frequently people remark that one form “seems” more effective, or that their lab results respond differently. That common observation is real, but its roots are more fascinating than most expect.
Vitamin D and the skeletal symphony: why osteoporosis prevention starts here
Osteoporosis isn’t only about bone density. It’s about bone remodeling—an ongoing negotiation between osteoclasts (the cells that break down bone) and osteoblasts (the cells that build it back). Vitamin D acts like a meticulous stage manager for this process. When vitamin D signaling is adequate, calcium absorption improves, mineralization becomes more efficient, and the remodeling cycle tends to stay within healthier boundaries.
In women, this story is especially urgent because estrogen fluctuations across life stages can accelerate bone turnover. Add age-related changes in skin synthesis and dietary patterns, and vitamin D adequacy can quietly drift downward. The skeletal consequences may appear later, after months of “small misses” have already accumulated. That’s why prevention feels like a long game—because it is.
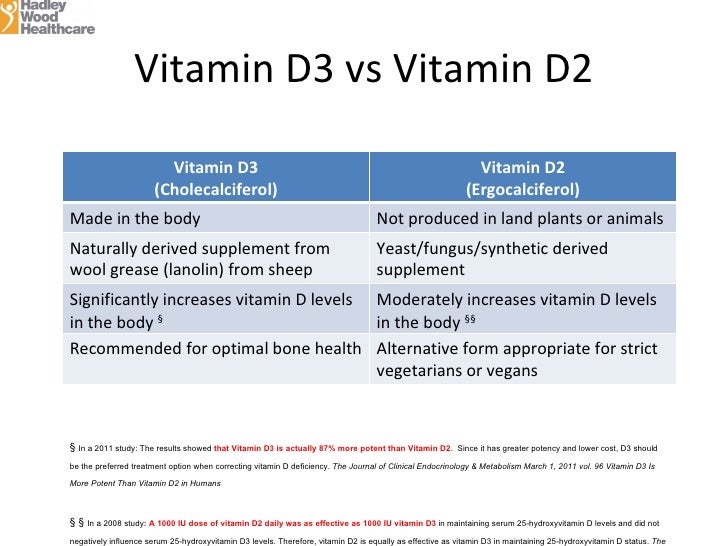
D3 vs D2 in plain language: two cousins, not identical twins
Vitamin D2 (ergocalciferol) and Vitamin D3 (cholecalciferol) both belong to the same family of fat-soluble secosteroids. Still, they aren’t mirror images. D3 is typically associated with sun exposure and animal-derived sources, while D2 is commonly found in certain fortified foods and plant-based supplements. That difference in origin matters because it hints at differences in how each form travels through the body and how it behaves once inside cellular chemistry.
Here’s the key takeaway women often sense: although both can raise vitamin D status, the magnitude and durability of that increase may diverge. The “why” becomes clearer when you consider absorption dynamics, conversion pathways, and the molecule’s biochemical persistence.
Absorption and bioavailability: the first hinge in the chain
After you ingest either form, your gut has to absorb it, then your body has to transport it to tissues that handle transformation. For many people, the form that is absorbed more efficiently (and perhaps packaged more favorably within dietary fats) can yield stronger downstream effects. This is partly why a supplement’s context—fat-containing meals, gut health, and dosing frequency—can shape how D2 or D3 “lands” in your system.
It’s tempting to assume that the body treats D2 and D3 identically at the outset. But physiology rarely rewards such simplicity. The gut environment is particular; bile availability influences lipid-soluble compounds; and individual variability can make one form feel “stronger” in practice.
Metabolism and activation: turning vitamin into an instruction
Vitamin D isn’t active immediately. It requires conversion steps, where liver enzymes and subsequent metabolic processing generate circulating metabolites that ultimately enable vitamin D receptor signaling. In many discussions, D3 is described as converting more effectively or maintaining higher circulating levels, though the details can vary by person.
Think of vitamin D as a letter. The first step delivers it to the right address; the second step makes sure it’s readable; the final step ensures the message reaches the correct cellular “mailbox.” When D3 tends to produce more stable, higher levels of circulating metabolites, that can translate into more reliable signaling for calcium handling and bone remodeling.
Storage and persistence: why D3 may feel like a longer promise
Because vitamin D is fat-soluble, it can accumulate in body compartments and be released gradually. This storage behavior contributes to how long blood vitamin D levels remain elevated after supplementation. Some women report that D3 “holds steady” better over time, and that perception aligns with the idea that D3 may have greater longevity in circulation for certain individuals.
Longer persistence isn’t just a convenience factor; it can mean more consistent receptor engagement, especially important for prevention strategies that rely on stability, not spikes. Bones respond to patterns. Intermittent correction may be less effective than sustained adequacy.
Clinical endpoints for osteoporosis prevention: beyond lab numbers
Lab results are a compass, not a destination. For osteoporosis prevention, what ultimately matters is fracture risk reduction and the preservation of bone microarchitecture. Bone is not simply “dense” or “light.” It has internal structure, resilience, and the ability to withstand stress cycles. Vitamin D supports mineralization and helps regulate the hormonal environment that influences bone remodeling.
Women often focus on 25(OH)D levels—an indicator of vitamin D status—but the deeper story includes how that status interacts with parathyroid hormone, calcium availability, and muscle function. Muscle strength influences fall risk, and fall risk is a major driver of fracture outcomes. In other words, vitamin D may protect bones indirectly by protecting mobility.
 Common observation: “D3 moved my numbers more” — and why that can happen
Common observation: “D3 moved my numbers more” — and why that can happen
Many people notice that D3 seems to raise vitamin D status more reliably than D2. That observation can be explained by differences in biochemical behavior after absorption, including metabolite patterns and how effectively each form contributes to circulating vitamin D measures. Some women find that D2 improves their levels but requires more frequent or higher dosing to reach the same target.
There’s also a narrative layer to consider: when someone feels better—less fatigue, improved muscle function, fewer aches—they may attribute it to the supplement, reinforcing the sense that one form “works better.” That subjective improvement can correlate with physiologic changes, but it can also be influenced by lifestyle factors that commonly travel with supplement use: increased outdoor time, improved nutrition, and adherence to overall wellness routines.
Women-specific considerations: menopause, body composition, and absorption variability
Menopause shifts the estrogen landscape, often accelerating bone loss. At the same time, body composition changes: fat distribution can increase, and that can alter vitamin D storage and mobilization. Because both D2 and D3 are fat-soluble, the storage and release pattern becomes more relevant.
Older adults may also experience decreased skin synthesis (less UVB conversion), changes in kidney function, and altered metabolism. If vitamin D activation efficiency or metabolite handling differs with age, the advantage of one form over the other may become more apparent.
Dosage realities: units, frequency, and the “too little” problem
The most common mistake isn’t the choice between D2 and D3—it’s under-dosing, inconsistent intake, or taking vitamin D without checking whether levels are adequate. Vitamin D needs vary by baseline status, sun exposure, diet, and body mass. For osteoporosis prevention, consistency is often more important than chasing dramatic short-term increases.
Some regimens use daily dosing; others use weekly or high-dose strategies. Women preparing a prevention plan should consider how their schedule affects adherence. A supplement that is technically effective but rarely taken is like an insurance policy you forget to renew.
Synergy and friction: vitamin D doesn’t work alone
Vitamin D is a facilitator. Calcium provides the building blocks, but without adequate vitamin D signaling, calcium absorption may lag. Magnesium and vitamin K also interact with bone metabolism pathways. When women choose a vitamin D strategy, they often need a bigger ecosystem: diet quality, resistance training, protein intake, and adequate sleep.
Here’s the friction point: some supplements are taken without consideration of interactions. High calcium without proper vitamin D can still leave absorption suboptimal. Excessive supplementation can also create issues. The most elegant approach is individualized, guided by testing and a clinician’s oversight when risk is elevated.
 Safety and monitoring: the careful art of staying within range
Safety and monitoring: the careful art of staying within range
Because vitamin D is fat-soluble, it can accumulate. That’s why monitoring matters, particularly for women with prior deficiency, kidney disease, or conditions affecting calcium balance. The goal is not maximal vitamin D—it’s sufficient, stable vitamin D activity that supports bone remodeling without overshooting.
A practical pattern is: supplement, recheck levels after an appropriate interval, and adjust. This turns guesswork into a measured prevention plan.
Choosing between D2 and D3: a decision framework for prevention
If the goal is osteoporosis prevention in women, many clinicians lean toward D3 due to frequent observations of stronger and more consistent increases in vitamin D status. Still, D2 can be appropriate in certain circumstances, including dietary preferences or availability. The decisive factors are not only the form but also the dosing strategy, adherence, baseline status, and your lab response.
Ask the deeper questions: Are you aiming for adequate maintenance or rapid correction? Are you taking it with food that improves absorption? Do you plan to monitor levels? Will your regimen support long-term consistency? Those answers tend to matter as much as the label.
The fascination underneath the difference: why this topic keeps resurfacing
Vitamin D2 vs D3 is fascinating because it illustrates a broader truth: small chemical differences can ripple into meaningful biological outcomes. It’s also a reminder that “common knowledge” often flattens complex systems into a single recommendation. Women who notice variations in response are not imagining it—they’re observing biology in motion.
Osteoporosis prevention is not one decision. It’s a sequence: ensuring vitamin D adequacy, supporting calcium and muscle function, and maintaining consistent lifestyle habits. When D3 or D2 is chosen wisely and tracked responsibly, the result isn’t just a better lab number. It’s a steadier foundation for bones that need endurance, not surprises.



