If you’ve started Wegovy and noticed something missing—perhaps a pause in the usual “checklist” conversations about vitamins—you’re not alone. Many clinicians focus on the immediate, visible priorities: titration schedules, gastrointestinal tolerance, and safety monitoring for weight-loss progress. But vitamin D is quietly relevant in the background. When it’s not addressed, it can feel like an oversight, even though the reason may be systemic, time-constrained, or rooted in differing clinical habits. Here’s what may be behind the silence, and what kinds of information you can reasonably expect to find when you seek clarity.
Why vitamin D sometimes gets deprioritized during Wegovy visits
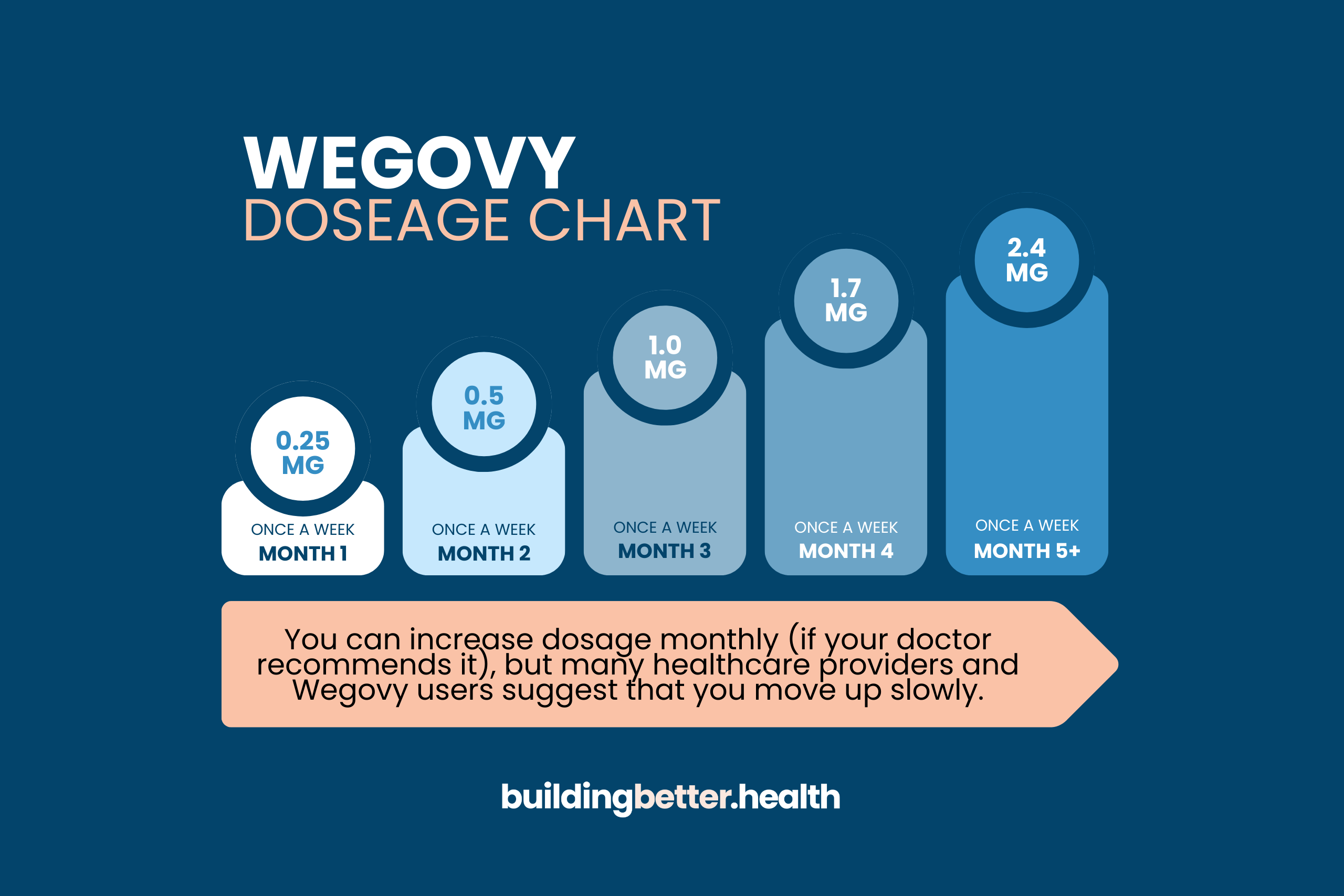
Wegovy appointments often become triage stations. The therapy has a distinct escalation pattern, and side effects can arrive like weather fronts—gradual at first, then more noticeable after dose increases. In that environment, clinicians may prioritize items that demand rapid attention: nausea, constipation, appetite changes, and signs that a different dosing strategy is needed.
Vitamin D, by contrast, is frequently an “under-the-surface” factor. Deficiency can exist without dramatic symptoms. Someone may feel “fine” while vitamin D remains low, especially in winter months, for people with limited sun exposure, and for those who spend most time indoors. When nothing seems urgently wrong, the conversation may drift away from less-immediate labs.
There’s also a workflow reality. Many practices rely on standardized protocols and may not automatically include every micronutrient in routine follow-ups for anti-obesity medications. That doesn’t mean it’s unimportant—it means it’s sometimes not embedded in the default path.
The metabolism of weight loss: vitamin D and shifting physiology
Vitamin D isn’t just about bones. It interacts with immune signaling, muscle function, and inflammation pathways. When body weight changes—especially through pharmacologic appetite reduction—physiology adapts. Fat mass can decline, which may influence how vitamin D is stored and released. That can create fluctuations that aren’t always predictable from day one.
Additionally, Wegovy can reduce overall intake. Even if you don’t “diet,” your plate may quietly shrink. Food that used to supply vitamin D—fatty fish, fortified dairy or alternatives, eggs—may become less frequent. The result is a subtle nutritional variability: not dramatic malnutrition, but a slow drift toward insufficient intake.
Sometimes the clinical eye stays on the scale, while vitamin D lives in the bloodstream, where the timeline is different. A person can lose weight steadily while micronutrient status worsens slowly enough to escape notice.
What “deficiency risk” actually looks like for different reader profiles
Not everyone faces the same probability of low vitamin D. When readers think “deficiency,” they often imagine a uniform group. In reality, the risk matrix is diverse.
People with darker skin tones may synthesize less vitamin D from sunlight. Those living in northern latitudes or spending most time indoors often have reduced UVB exposure. Individuals with malabsorption conditions—such as celiac disease, inflammatory bowel disorders, or certain pancreatic or liver issues—may have difficulty absorbing fat-soluble nutrients.
Older adults can be vulnerable too. Aging can reduce the skin’s efficiency at producing vitamin D and can also alter how the body activates it. Readers who are pregnant, post-menopausal, or managing chronic kidney or parathyroid disorders may need a more careful, individualized approach.
Even lifestyle can matter: clothing coverage, sun-avoidance habits, and the use of broad-spectrum sunscreen can all reduce vitamin D generation. None of these are “faults.” They’re simply variables that influence biochemical outcomes.
How vitamin D connects to safety monitoring—and why the conversation may lag
Clinicians commonly monitor calcium, kidney function, and sometimes other metabolic markers when specific conditions are present. But vitamin D testing isn’t always routine for every patient on Wegovy. If the medication start is already laden with labs and follow-ups, vitamin D can be perceived as optional.
Yet vitamin D deficiency can intersect with other concerns. Bone health, muscle performance, and fracture risk matter across weight-loss strategies. Deficiency can also complicate symptoms that readers may attribute to “just the medication”—fatigue, generalized aches, or reduced resilience during exercise.
Because those symptoms are nonspecific, they can be misclassified. It’s easier to interpret them as a gastrointestinal aftermath than to consider a nutritional insufficiency. That mismatch is a common reason vitamin D discussions don’t show up early.
Different types of content readers can expect to find
When people search for vitamin D while using Wegovy, the information landscape tends to fall into several formats—each with its own strengths and blind spots.
1) Dosing guidance explainers
You’ll often see content that focuses on supplementation basics: daily versus weekly dosing, typical ranges, and the concept of correcting deficiency versus maintaining adequate levels. These pieces are usually helpful, but they may be overly generalized.
2) Lab interpretation and “numbers” breakdowns
Some readers prefer content that translates bloodwork into plain language. These articles may explain vitamin D’s circulating form (25-hydroxyvitamin D), and how clinicians interpret severity. The best versions also remind readers that individual targets can vary with age, comorbidities, and baseline risk.
3) Meal-based or “food-first” content
Other readers want practical food strategies: fortified options, cooking methods that improve intake, and how to maintain micronutrient density when appetite is lower. This category often includes meal ideas and shopping lists. It can be especially useful when medication reduces the capacity to eat consistently.
4) Safety and interaction content
A smaller but crucial genre focuses on the hazards of overcorrection—particularly hypercalcemia risk when doses are excessive or when people have certain medical conditions. These pieces often read as cautionary checklists, and they’re valuable for grounding supplement use in restraint.
5) “Personal narrative” experiences
Some content is story-driven: how a patient discovered deficiency after fatigue appeared, or how an adjustment improved energy and training tolerance. Narratives can be emotionally resonant. They also require caution, because one person’s outcome isn’t a universal template.
What to ask your doctor when vitamin D isn’t mentioned
If your clinician hasn’t raised vitamin D, you can make the conversation specific. Consider asking whether you’re a good candidate for a 25-hydroxyvitamin D test, especially if you have limited sun exposure, bone issues, or risk factors for malabsorption. You can also request a brief strategy for supplementing—if needed—based on anticipated intake changes from Wegovy.
Another useful question is how vitamin D fits with a broader plan for bone health: strength training, dietary calcium adequacy, and monitoring timelines. Short, targeted questions often work better than broad prompts. Instead of asking, “Should I take vitamin D?” try, “Given my risk factors and weight-loss timeline, should we check my level and plan a maintenance dose?”
Finally, ask what symptoms should trigger follow-up. That creates a shared safety map and reduces the chance that vague discomfort will be dismissed.
Practical steps for readers: build vitamin D into a Wegovy routine
Even without a direct mention from a doctor, readers can take practical steps that don’t require panic. One approach is to track sunlight exposure patterns seasonally and note dietary sources of vitamin D. Another is to plan fortified foods into meals when appetite is suppressed—because micronutrient intake often drops faster than people expect.
Supplements can also be considered, but restraint matters. The goal is usually adequacy, not megadoses. Too much vitamin D can push calcium levels upward, which can become medically significant. A clinician’s input—or at least lab-based guidance—is the most reliable route.
If your healthcare team has you on labs already, consider aligning vitamin D testing with other monitoring. That way, information is collected efficiently, and decisions become evidence-guided rather than guesswork.
When vitamin D conversations should become urgent
Urgency isn’t about alarm—it’s about signals. If you experience persistent muscle weakness, frequent bone pain, unusual fatigue that doesn’t track with titration side effects, or you have known osteoporosis or fractures, vitamin D should move higher on the priority list. People with kidney disease, parathyroid disorders, or a history of high calcium should also be especially careful.
In those cases, waiting for the “next routine conversation” can be inefficient. It’s reasonable to request targeted evaluation. Precision is not a luxury; it’s risk management.
The real takeaway: silence isn’t denial
When vitamin D isn’t mentioned during Wegovy initiation, it may reflect time constraints, protocol design, or an assumption that supplementation and labs are already handled elsewhere. It doesn’t automatically mean vitamin D is irrelevant. Often, it means the conversation hasn’t been structured yet.
As weight-loss treatments evolve, micronutrients should remain part of the narrative. The most effective care is the kind that connects dots: appetite reduction, dietary variability, bone and muscle maintenance, and lab-guided adjustments. If vitamin D hasn’t entered your story, you can help write that chapter—calmly, specifically, and with the right questions.




