
Picture your body as a meticulous warehouse. When you take vitamin D—whether as D2 (ergocalciferol) or D3 (cholecalciferol)—you’re essentially deciding how efficiently that warehouse can store, circulate, and keep inventory available. One of the most practical ways to understand that process is through a concept called half-life. It’s not just an academic detail; it can influence how long vitamin D stays “active” in your system, how quickly levels rebound, and how your supplementation plan may feel over time.
Half-Life, Explained Without the Lab Coat
Half-life is the time it takes for the concentration of a substance in your bloodstream to drop by 50%. With vitamin D, “dropping” doesn’t mean the vitamin vanishes instantly. Instead, levels gradually decline as the body metabolizes and redistributes it. This timeframe matters because vitamin D isn’t a fleeting nutrient; it’s a secosteroid hormone precursor with roles in calcium homeostasis, immune modulation, and bone metabolism.
Short sentences help: half-life equals “how long the signal persists.” Long sentences help too: the persistence of vitamin D in circulation is tied to your baseline status, liver processing, and the downstream production of active metabolites.
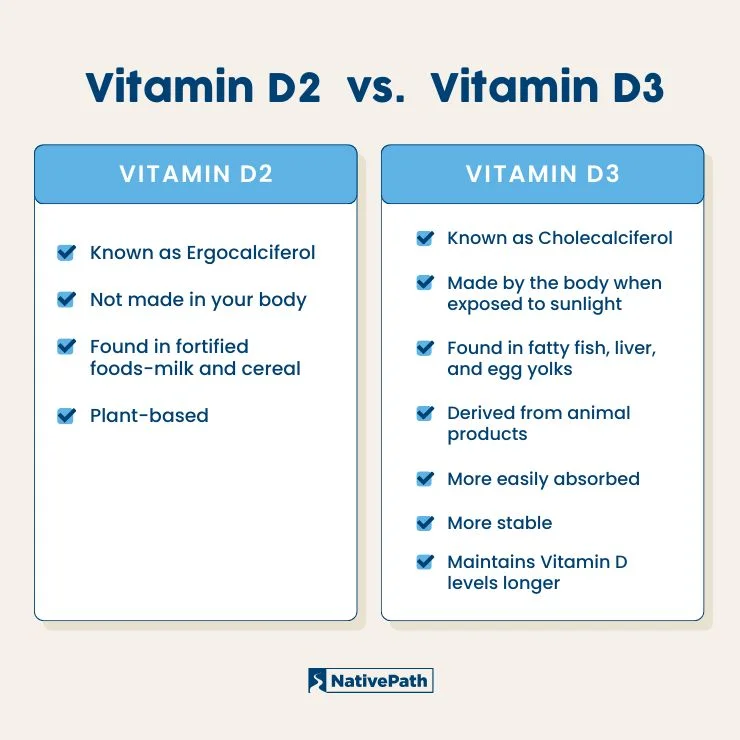
Vitamin D2 vs D3: A Quick Identity Check
Vitamin D2 typically comes from plant sources and is synthesized industrially in ways that mirror those origins. Vitamin D3 is produced by skin in response to UVB exposure and is also available through animal-based dietary sources or specialized supplements.
Both forms can raise vitamin D levels, but their biochemical behavior can differ. Many people notice these differences not as a feeling, but as a pattern: how consistent their blood levels stay after a course of supplementation, and how rapidly their numbers drift downward between doses.
The Half-Life Difference: Why It Can Matter in Real Life
When people discuss “vitamin D3 vs D2 half-life,” they’re usually reacting to a practical observation: vitamin D3 tends to maintain 25-hydroxyvitamin D levels more robustly over time than vitamin D2 for many individuals. The phrase “half-life” is a shorthand for that reality—how quickly the measured circulating reservoir decreases after supplementation.
Here’s the nuance: half-life data can vary depending on assay methods, baseline vitamin D status, dose, and how the body handles absorption and metabolism. Still, the pattern is clinically meaningful. If D3 clears more slowly, it may provide a steadier therapeutic runway—especially for people who supplement intermittently.
What Your “25(OH)D” Level Is Doing Behind the Curtain
The biomarker most clinicians track is 25-hydroxyvitamin D, abbreviated as 25(OH)D. Think of it as the body’s storage-and-delivery ledger. Vitamin D2 and D3 are processed in the liver, and from there they can be converted into more active forms that influence physiology.
Half-life influences the slope of that ledger. A longer effective persistence means your 25(OH)D may decline more slowly, which can affect whether you remain within an optimal range from one blood test to the next.
In storytelling terms: D2 and D3 might both start the same journey, but they can take slightly different routes through the body’s metabolism, and those routes determine how long your vitamin D “plot” stays interesting.
Dose Timing: How Half-Life Shapes Your Supplement Routine
Half-life is not just about what happens after you stop taking vitamin D—it’s also about how you schedule when to take it. If a form declines faster, a person may need more frequent dosing or higher total intake to prevent troughs. If a form declines more slowly, longer intervals might still keep levels stable.
Short version: D3 may “bridge gaps” better for some people. Longer version: stable levels can reduce the risk of seasonal dips, especially during winter months when sun exposure drops and dietary intake becomes less reliable.
Loading Doses vs Steady Maintenance: Different Strategies, Different Feelings
Some supplementation protocols use a loading phase to raise levels quickly, followed by a maintenance phase. Half-life considerations can influence how aggressively a loading phase is designed and how long the maintenance phase must continue.
If D2 declines more rapidly for an individual, a maintenance plan may need recalibration. If D3 maintains levels more consistently, maintenance might be smoother, requiring fewer “rescue” doses.
In practice, this affects patient experience: fewer roller-coaster lab results, fewer adjustments, and less cognitive fatigue from wondering whether today’s dose “counts” tomorrow.
Absorption and Bioavailability: The Secret Room Adjacent to Half-Life
Half-life is one part of the story, but absorption is another gate entirely. Vitamin D is fat-soluble, meaning it often benefits from taking it with a meal containing fat. Gut health, body composition, bile flow, and medication interactions can all influence absorption.
Two people can take the same vitamin form and dose, yet their measured 25(OH)D trajectory diverges. Half-life may determine how long it sticks, but absorption determines how much sticks in the first place. Together, these factors shape your real-world half-life effect.
Uncommon terminology, but useful: consider “pharmacokinetic persistence,” which is essentially the experiential version of half-life—how long your body keeps the vitamin available for biochemical tasks.
Who Might Notice the Half-Life Difference More?
Half-life differences may be more noticeable for people who:
• Take vitamin D intermittently rather than daily
• Have low baseline 25(OH)D and are repleting stores
• Live in regions with limited UVB exposure
• Have conditions that affect absorption (for example, certain gastrointestinal disorders)
• Have higher body mass index, which can influence vitamin D distribution into adipose tissue
When baseline levels are low, the rebound arc can be steep. When baseline levels are already adequate, maintenance becomes the main challenge—and that’s where the “how slowly it falls” question becomes quietly important.
Blood Test Interpretation: Don’t Confuse Time Lag With Failure
After changing a vitamin D regimen, lab results may not respond instantly. There’s a time lag because vitamin D processing and conversion take time, and your body needs enough duration to reach a new equilibrium. Half-life affects the slope of decline and the speed of rebalancing, but interpretation requires patience.
Consider it like tuning an instrument. If you check the sound too quickly, it may look off—not because the method is wrong, but because the system hasn’t finished settling.
Safety, Upper Limits, and the Half-Life “Trap” to Avoid
More persistence doesn’t automatically mean “more is better.” Vitamin D can accumulate if dosing is excessive, particularly with high-dose regimens used without follow-up. Because D3 may maintain levels more effectively for many individuals, it’s critical to align dosing with professional guidance and periodic monitoring.
Safety isn’t only about half-life; it’s also about total dose, co-factors like calcium intake, and the presence of kidney issues. Unusually high vitamin D levels can increase calcium and create complications. The goal is balance, not dominance.
Choosing Between D2 and D3: A Practical Decision Framework
Think of this as a decision tree rather than a battlefield. Ask:
• What’s your baseline 25(OH)D status?
• Are you aiming for repletion or maintenance?
• How consistent can you be with dosing?
• Do you take it with meals that contain fat?
• Are you monitoring levels periodically?
For many people, D3 tends to be the more favorable option when steady maintenance is the objective. For others—based on availability, preference, or clinician recommendation—D2 may still be effective. The key is alignment between form, half-life behavior, and your lifestyle rhythm.
What Content Readers Can Expect Going Forward
If you continue exploring this topic, you’ll encounter several content “types,” each with its own usefulness:
1) Nutrient chemistry explainers: These focus on molecular identity, metabolism in the liver, and conversion pathways. They’re great for understanding why half-life might differ.
2) Clinical interpretation guides: These translate lab results into practical steps—how to time retesting and how to adjust dosing.
3) Lifestyle optimization pieces: These connect vitamin D intake to sunlight exposure, diet, meal timing, and consistency habits.
4) Safety-focused explainers: These emphasize monitoring, contraindications, and upper intake cautions—especially for high-dose regimens.
5) Myth-busting content: These address overconfident claims such as “one form always wins” or “vitamin D never matters if you’re outside sometimes.” Reality is more nuanced.
Your Takeaway: Half-Life as a Compass, Not a Verdict
Vitamin D3 vs D2 half-life is best understood as a compass pointing toward how reliably your body maintains vitamin D stores over time. For many individuals, D3’s persistence can translate into more stable 25(OH)D levels, smoother maintenance, and fewer dips between doses. Yet the “best” choice still depends on baseline status, absorption, dosing consistency, and monitoring.
If you want one sentence to keep: treat half-life as a guide for designing your regimen—then let data (your blood work) confirm the route.




