
For years, migraine has felt like an unwelcome weather system—sometimes quiet, sometimes violently seasonal. In the middle of that unpredictability, a quieter variable has been drawing renewed attention: vitamin D, particularly the rivalry between D2 and D3. Recent discussions in the clinical world suggest that the “form” of vitamin D may matter more than many people assumed, especially when the goal is migraine prevention rather than general wellness.
Why Vitamin D Shows Up in Migraine Conversations
Migraine prevention is rarely a single-pathway story. It’s more like a chorus of biochemical signals—neuronal excitability, inflammatory tone, immune modulation, and vascular reactivity. Vitamin D, while often framed as a bone nutrient, also behaves like a neuroimmunological regulator. That’s one reason researchers keep returning to it.
Newer reasoning focuses on plausibility: vitamin D influences inflammatory cytokines, modulates oxidative stress responses, and may affect the synthesis of neuroactive compounds. If those pathways contribute to migraine susceptibility, then correcting deficiency could plausibly reduce attack frequency or severity.
What’s changed most recently is not just the interest in vitamin D itself, but the attention to which vitamin D is being administered. D2 and D3 are not identical guests at the biochemical table—they may be absorbed, metabolized, and utilized differently.
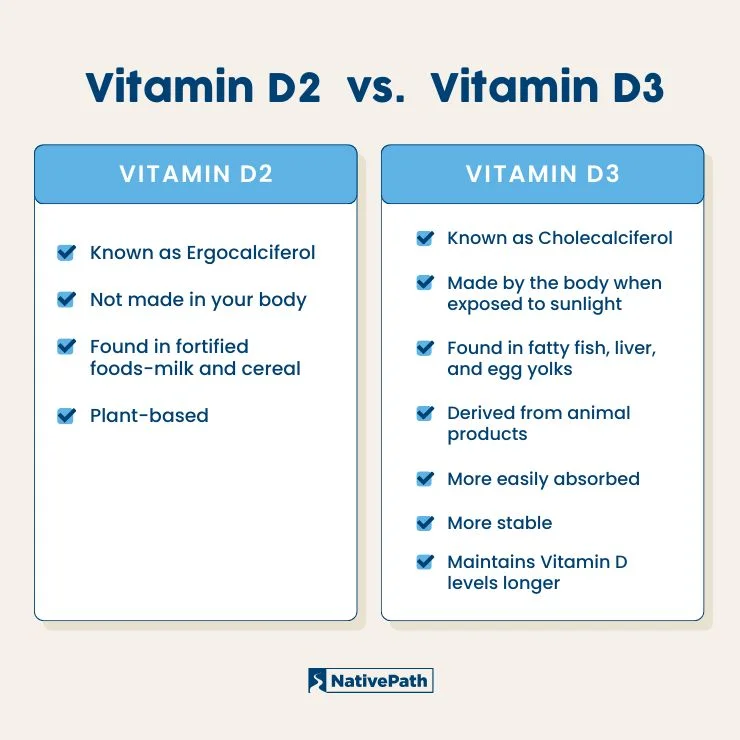
D2 vs D3: The Biological Differences That Matter
Vitamin D2 (ergocalciferol) is typically sourced from plant-based fungi. Vitamin D3 (cholecalciferol) is commonly derived from animal sources or produced via microbial synthesis. Both can raise blood levels of vitamin D metabolites, but the downstream choreography can differ.
D3 often exhibits a stronger ability to maintain circulating vitamin D status over time. The reason is tied to how each form is processed in the liver and converted into active metabolites that interact with vitamin D receptors. In migraine prevention, duration and stability of vitamin D levels may be more important than short-lived spikes.
Consider this as a difference between a brief light flicker and a steady illumination. If migraine-related pathways require consistent regulation—particularly in people who are deficient or borderline—D3 may provide a more dependable baseline.
What “New Research” Is Reframing
Across emerging discussions, the narrative is shifting from simple supplementation to targeted reasoning. Instead of asking, “Does vitamin D help migraines?”, the modern questions sound more precise: “Which form helps most?” and “In whom does supplementation yield measurable benefit?”
Some findings and analyses emphasize that D2 may be less robust in raising or maintaining sufficient circulating levels compared with D3. Others highlight that people with vitamin D deficiency may respond better than those with adequate baseline status. In other words, the same supplement can yield different outcomes depending on starting physiology.
That’s why current research conversations increasingly consider vitamin D status measurements, treatment duration, and adherence—because migraine is notorious for punishing inconsistent schedules.
How Vitamin D Status Is Measured (And Why It’s Not a Detail)
When clinicians and researchers talk about vitamin D, they usually refer to serum 25-hydroxyvitamin D. This marker is the most commonly used gauge for vitamin D stores. A person can appear “healthy” while still running low, which makes the deficiency variable both silent and influential.
If someone begins supplementation without assessing baseline levels, it can be hard to interpret results. A “responders vs non-responders” divide often emerges when deficiency is not documented. With migraine prevention, that divide matters—because migraines may be influenced by a threshold phenomenon.
Imagine a dimmer switch rather than an on/off switch. If vitamin D helps tune immune and neuronal signaling, then insufficient levels might leave the system under-adjusted.
Mechanisms: How D3 Could Be More Migraine-Relevant
Vitamin D engages with vitamin D receptors found in multiple tissues, including components of the immune system and potentially relevant neural pathways. This creates a plausible bridge between vitamin D metabolism and migraine physiology.
D3’s stronger persistence may enhance receptor activation over time. That matters because migraine prevention isn’t just about extinguishing inflammation for a day—it’s about recalibrating the underlying “irritability” of neural circuits and immune signaling networks.
In practical terms, D3 may better sustain the biochemical conditions associated with fewer migraines. The effect may not be immediate; it can resemble slow weathering—subtle early changes that later become clinically noticeable.

Who Might Benefit Most: Deficiency, Risk, and Phenotype
Not all migraine is the same. Some people experience migraines with aura; others have chronic patterns. Triggers differ, hormonal influences vary, and comorbidities—like sleep disturbance or inflammatory conditions—can alter response.
Vitamin D deficiency is more common in individuals with limited sunlight exposure, darker skin pigmentation, higher body mass index, older age, or certain dietary patterns. If migraine susceptibility intertwines with deficiency-driven immune imbalance, then these groups may be disproportionately likely to benefit from correcting vitamin D inadequacy.
However, supplementation is not a universal solvent. Some patients may need a broader preventive strategy that includes sleep hygiene, trigger management, and—when appropriate—evidence-based pharmacologic prophylaxis.
Dosage, Timing, and Safety: A Practical Consideration
Choosing between D2 and D3 isn’t merely academic; it influences how you plan dosage and monitor results. Many clinicians prefer D3 for the goal of achieving and maintaining stable serum levels. Still, dosing should be individualized and guided by lab values.
Safety is essential. Excess vitamin D can contribute to hypercalcemia and related complications. That’s why follow-up testing and adherence to dosing guidance are important. Short-term experimentation can be tempting, but migraine prevention is a long game.
Many people find that consistent dosing—rather than sporadic high doses—supports better biological stability. Whether using daily, weekly, or other regimens, the key is consistency and monitoring.
What Content Readers Often Need Next: Side-by-Side Guidance
Readers typically want clear comparisons they can apply. A practical way to organize this topic is to expect content that includes: a summary of which form tends to perform better for maintaining serum vitamin D, what the likely mechanisms are, and who should prioritize getting tested.
It also helps when articles provide “decision scaffolding,” such as: steps to discuss testing with a clinician, how to interpret lab results, and what timeframe to consider when evaluating migraine response. Short sentences are helpful here—because the mind wants a map when symptoms feel foggy.
At the same time, long-form narrative sections matter. They let readers understand why the physiology isn’t magic and why migraine prevention often behaves like a slow remodeling process.
Setting Expectations: How Long Until Migraine Changes Are Noticeable?
Migraine improvement, when it occurs, may not arrive overnight. Vitamin D functions through receptor-mediated changes and immune modulation—processes that require time. Many preventive interventions show a delayed effect, and vitamin D should be approached with that same realism.
A reasonable content expectation is to see timelines discussed: weeks for biochemical changes, longer for symptom patterns to shift. Keeping a headache diary during this period can help connect dosage decisions to actual migraine outcomes.
Not every patient will experience meaningful reduction. Some will notice smaller improvements in severity or resilience to triggers. Others may see no change, which does not invalidate the concept; it simply means migraine is multifactorial.
The Bottom Line for Migraine Prevention: Choosing D3 with Intelligence
Vitamin D3 is frequently favored in modern discussions because it appears to better support sustained vitamin D status—an attribute that aligns with the longer horizon required for migraine prevention. D2 can still be useful, but the emerging emphasis is on effectiveness, persistence, and how reliably serum levels are maintained.
Ultimately, the most important decision is not only D2 versus D3. It’s whether vitamin D status has been assessed, whether supplementation is appropriately dosed, and whether the plan fits into a comprehensive migraine-prevention strategy.
When vitamin D is chosen intelligently—paired with testing, safety monitoring, and realistic timelines—it becomes less of a supplement and more of a structured support for neuroimmunological balance.




