
Imagine vitamin D as a letter written in two different inks. One ink is crafted in your skin under sunlight, unfolding its meaning the moment rays arrive. The other ink is carried in a capsule, arriving already formed—promising convenience, predictability, and control. But the question remains: is the “bioactivity” actually different? In other words, does sun-made vitamin D behave the same way once it enters your physiology, or does the route of delivery sculpt its effects in subtle, sometimes surprising ways?
The Journey Begins: Two Paths, One Destination
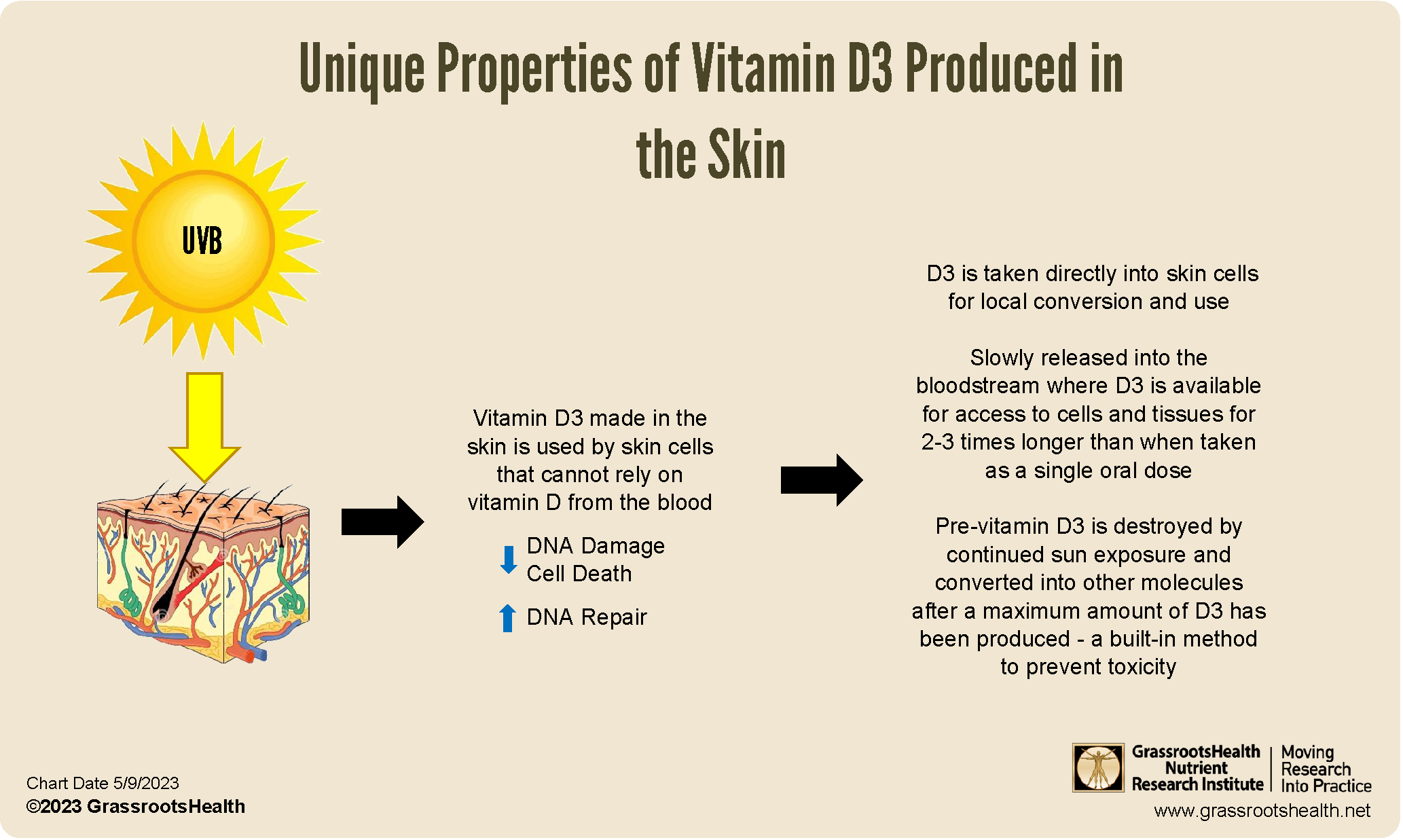
Vitamin D can be produced in the skin when ultraviolet B (UVB) light converts a precursor molecule into vitamin D3 (cholecalciferol). Oral D3 bypasses the skin’s conversion step and delivers vitamin D3 directly into the bloodstream through the digestive process. Both routes ultimately converge at a functional bottleneck: the liver and kidneys “edit” vitamin D into its circulating hormonally active forms—especially calcitriol, the classic signaling molecule that influences calcium balance, bone mineralization, and a host of immune-modulatory pathways.
Think of this like two scenic train routes that both end at the same central station. The landscape differs—stations, delays, and scenery—but the travelers still step onto the final platform. Bioactivity, therefore, may be less about the origin story and more about how efficiently each body moves from raw material to functional output.
Bioactivity Defined: What You’re Really Measuring
“Bioactivity” is not a single switch—it is a choreography of conversion, transport, receptor binding, tissue availability, and downstream gene expression. When people compare sun versus oral D3, they often focus on blood levels of 25-hydroxyvitamin D (25(OH)D), the storage/transport marker. But biological outcomes depend on multiple layers beyond that measurement.
Short sentences help here: the body is not a vending machine. It is a living library with multiple copies of the same book, different editions, and different reading rooms. Calcitriol levels, vitamin D receptor (VDR) engagement, and the interaction with binding proteins (such as vitamin D–binding protein) all influence the “felt” effects.
So, any difference between sun and oral D3 would likely appear in these layers—how much gets made, how consistently it gets made, and how the body calibrates conversion based on context.
Sunlight’s Advantage: A Dynamic, Self-Regulating Input
Sun exposure is inherently interactive. Your skin receives UVB, synthesizes vitamin D3, and simultaneously responds with other photobiological effects—some helpful, some unrelated, some complex. The process is also sensitive to variables like latitude, season, cloud cover, time of day, skin pigmentation, age, body surface area exposed, and even sunscreen use.
This variability can feel inconvenient, yet it also suggests a kind of physiological “adaptation.” The body may adjust conversion steps and regulate vitamin D activation depending on the current environment. In narrative terms, sunlight is like a drumbeat: irregular, sometimes loud, often responsive. Oral D3, in contrast, is a steady metronome.
However, the dynamic nature of sunlight can cut both ways. A cloudy week or heavily sun-protected routine might cause an abrupt drop in vitamin D production—then the system has to recover later. Oral D3 tends to be more consistent, and consistency can support steadier biochemical conditions.
Oral D3’s Advantage: Precision and Predictability
Oral D3 resembles an engineered delivery system: you ingest a known quantity of vitamin D3, which is then absorbed and transported. While absorption can vary—fat intake, gut health, bile availability, and medication interactions all matter—many people experience more predictable rises in 25(OH)D compared with the feast-or-famine pattern of sun exposure.
Predictability can be powerful for bioactivity because downstream conversion processes often respond to adequate substrate availability. When the body has enough “raw material,” it can produce active forms more reliably. That’s not a guarantee of uniform effects—individual biology is still variable—but it supports a stable biochemical baseline.
In metaphor terms, oral D3 is a supply chain: it delivers inventory in a scheduled way. Sunlight is a weather event: productive when conditions are favorable, silent when they aren’t.
Is the Active Form Different? The Convergence Argument
Here’s the central point: both sun-produced vitamin D3 and oral vitamin D3 are chemically identical as vitamin D3. After that, the body’s conversion steps—first in the liver and then in the kidneys—operate on the molecule itself. If the substrate is the same, the enzymatic “editing” is guided by your physiology rather than by the molecule’s origin.
So, the likelihood of a meaningful difference in bioactivity is reduced by this convergence. The body is not likely to treat vitamin D3 as a different species because it entered through sunlight versus a capsule. Still, origin can influence the timing and consistency of substrate availability, which can indirectly shape bioactivity outcomes.
In other words: the molecule’s identity likely stays constant, but the rhythm of delivery may alter the overall physiological narrative.
Timing Matters: Rapid Peaks vs. Gradual Accretion
Sun exposure can create fluctuating vitamin D levels—sometimes with noticeable increases shortly after sufficient UVB exposure. Oral supplementation often produces a smoother trend depending on dosage frequency. Over time, these patterns may influence how frequently tissues experience adequate 25(OH)D concentrations.
Bioactivity is frequently about exposure context. A receptor-driven process does not only care whether a ligand exists; it also considers how steadily it arrives. Some biological pathways may respond better to steadier availability, while others may be less sensitive to the shape of the curve.
Short and sharp: the body is sensitive to kinetics. The result may not be a fundamentally different active chemistry, but it can be a different physiological experience.
Tissue-Level Effects: Why “Same Blood Level” Can Still Feel Different
Even with similar measured 25(OH)D levels, individuals can display different outcomes. Factors such as VDR expression, genetic variability in vitamin D metabolism, inflammation status, adiposity (which can sequester vitamin D), and differences in binding protein capacity can alter how much active signaling reaches target tissues.
Thus, sun versus oral D3 is only one axis. Another axis is the terrain: the microbiome, liver and kidney function, baseline metabolic health, and lifestyle factors that influence conversion and responsiveness.
To keep the metaphor: two people can have the same number of keys, but different locks. The “bioactivity” is the unlocking event, not just the key count.
Safety and Risk: The Cost of an Overzealous Sun
Sunlight provides vitamin D but also ultraviolet radiation with well-established risks. Excess UV exposure increases the probability of skin damage and long-term complications. So, even if sunlight and oral D3 eventually share the same mechanistic core, the safety profile of “getting vitamin D” from sun exposure is not identical to supplementation.
Oral D3 shifts the risk equation away from UV harms. Still, dosing matters: too much vitamin D can lead to hypercalcemia and related complications. The professional approach is not ideology—it is titration, monitoring, and individualized decision-making.
Immune Modulation and Beyond: What Research Often Emphasizes
Vitamin D is commonly discussed in the context of immune function, inflammation modulation, and cell signaling. Yet outcomes vary between studies, partly because populations differ in baseline deficiency status, adherence, dosage strategies, and outcome definitions. The route of vitamin D acquisition may not be the dominant determinant of immune effects once adequate circulating levels are achieved.
If there is a difference, it is more likely to be indirect—through consistency, timing, overall dose delivered, and co-factors that travel with the sun lifestyle versus a supplement routine—rather than through a unique vitamin D molecule generated only by sunlight.
Long sentences can blur into one idea: the immune system is exquisitely context-dependent.
So, Is There a Difference in Bioactivity Between Sun and Oral D3?
Most evidence-driven reasoning points toward a nuanced answer: the vitamin D3 produced by sun and the vitamin D3 taken orally are the same chemical form, and both are subject to the same activation machinery. That means the core bioactivity—particularly once the active metabolites are produced—should be broadly comparable.
However, differences can still emerge from the “delivery system.” Sun exposure introduces variability in dose and timing, influenced by geography, skin characteristics, and behavior. Oral D3 often provides more control over dosing and consistency, but absorption can vary based on digestive factors and overall health.
Bioactivity, therefore, is not only about origin. It is about how efficiently the body receives, converts, and deploys vitamin D across time—like an orchestra where the instruments may be identical, but the rehearsal schedule and conductor’s tempo change the performance.
Practical Takeaway: Choosing the Route That Fits the Body and the Calendar
A thoughtful approach respects both physiology and reality. If you can safely obtain sunlight in a way that aligns with your skin type and risk tolerance, it can contribute to vitamin D status. If predictability is important—during seasons with limited UVB, in indoor-heavy routines, or when exposure is constrained—oral D3 can be a pragmatic option.
Ultimately, the best route is the one that helps maintain adequate vitamin D status without trading away safety. Measuring 25(OH)D and discussing dosing strategies with a qualified clinician can turn the metaphor into a map: not just “sun versus supplement,” but “how to reach functional adequacy for your specific biology.”





