
When the ovaries become restless—altering follicle development, hormone rhythms, and the delicate choreography of ovulation—many people wonder what else might be quietly involved. Vitamin D is one such suspect. It’s often discussed in the context of bones and sunshine, yet its influence reaches further, into immune signaling, cellular differentiation, and reproductive endocrinology. Emerging evidence suggests that vitamin D deficiency may be associated with ovarian cyst formation and with broader ovarian dysfunction, especially in patterns resembling polycystic ovary syndrome (PCOS). The relationship isn’t a simple one-to-one chain. It’s more like a web: hormones, inflammation, metabolic factors, and ovarian microenvironment all interlace.
Vitamin D: More Than a Sunshine Nutrient
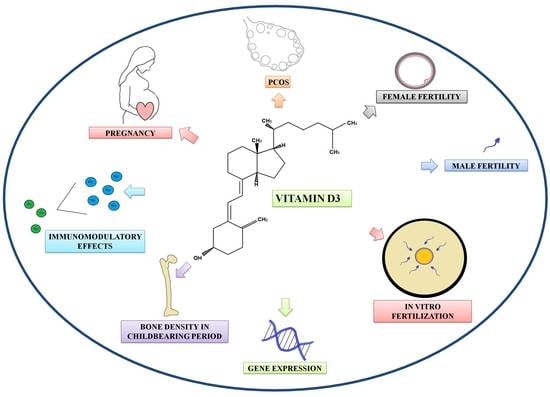
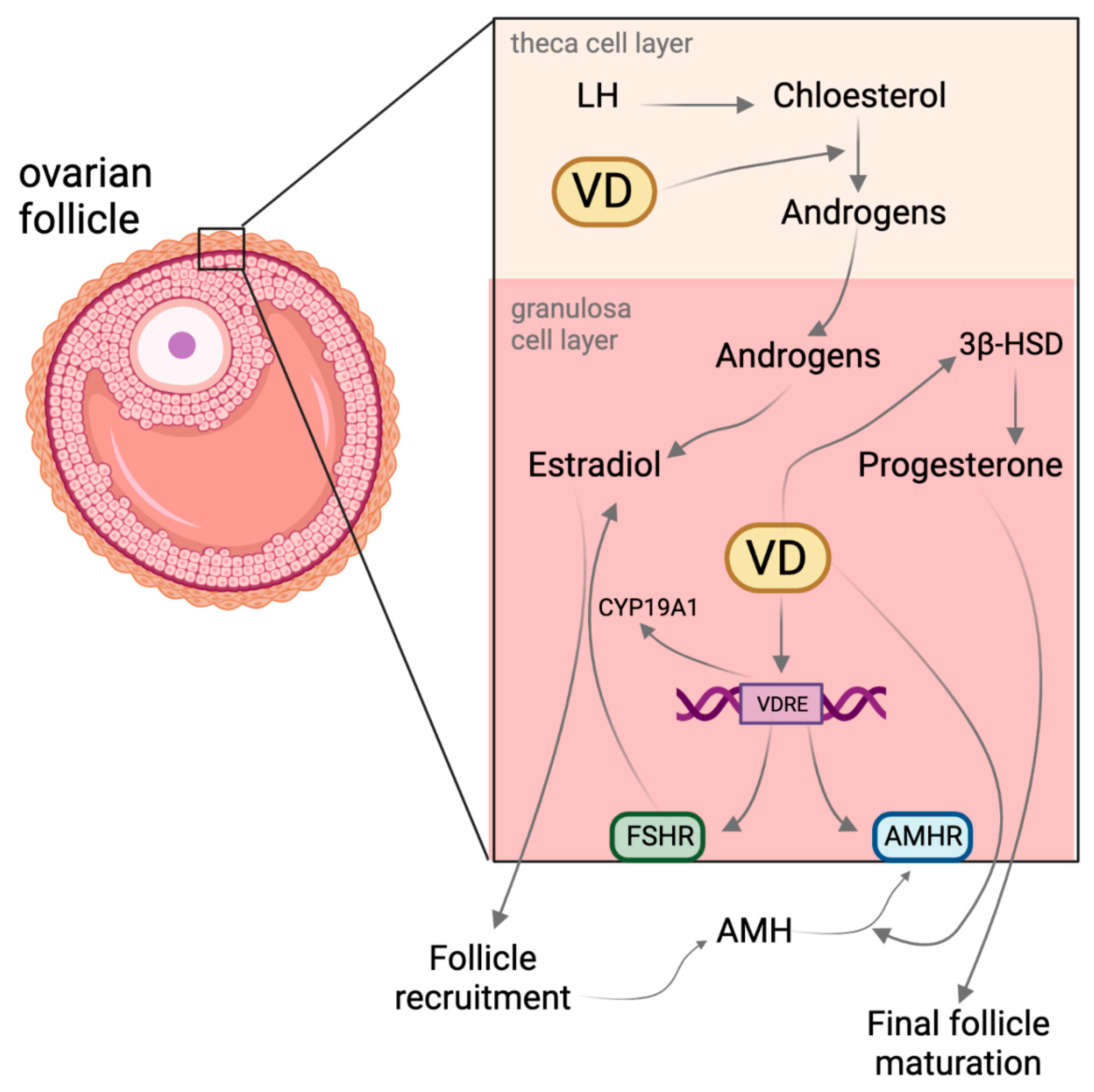
Vitamin D behaves less like a vitamin and more like a hormone precursor—steering gene expression through the vitamin D receptor (VDR) found in many tissues, including reproductive organs. Think of it as a molecular “switchboard operator” that nudges cells toward particular behaviors. In the ovaries, this signaling can affect granulosa cells, follicular growth, and steroidogenesis. Small changes in vitamin D status may therefore ripple outward, altering how follicles mature and how the ovarian environment handles oxidative stress.
Vitamin D also participates in immune modulation. That matters because ovarian cysts—particularly those linked with chronic dysfunction—often travel with inflammatory undertones. Not every cyst is the same, and not every person’s physiology responds identically. Still, a deficiency can tilt the balance toward higher inflammatory signaling and impaired metabolic homeostasis, both of which can influence ovarian function.
Understanding Ovarian Cysts: Functional vs. Pathological
To interpret the vitamin D story, it helps to separate ovarian cysts into broad categories. Functional cysts are tied to normal cycles—follicular cysts and corpus luteum cysts. They often resolve spontaneously. Pathological cyst patterns are more entwined with underlying endocrine or metabolic issues, and they may persist or recur.
While functional cysts can appear even in healthy cycles, chronic patterns like those in PCOS can involve multiple small follicles that fail to mature properly. In that setting, vitamin D may intersect with the mechanisms that govern follicle selection and ovulation timing. The question becomes not just whether vitamin D is “present,” but whether its signaling pathways are adequate for optimal ovarian regulation.
Vitamin D and PCOS: Where the Discussion Intensifies
PCOS is often characterized by androgen imbalance, irregular ovulation, and polycystic ovarian morphology. Many people describe it as a cyst-related condition, though clinically it’s more accurately an ovulatory and endocrine disorder. Here, vitamin D becomes particularly relevant because PCOS frequently overlaps with insulin resistance, low-grade inflammation, and dysregulated ovarian follicle development.
When vitamin D levels run low, ovarian and metabolic pathways may become less efficient at maintaining equilibrium. Insulin resistance can amplify androgen production, while inflammation can disrupt follicular maturation. Vitamin D signaling intersects with both fronts—potentially improving insulin sensitivity and calming inflammatory cascades. The net effect, in some individuals, may be improved ovulatory function and more regular cycles, which can indirectly reduce the appearance of cyst-like patterns.
Possible Mechanisms: How Vitamin D Might Influence Cyst Formation
Science rarely offers a single lever; it usually offers a cluster of mechanisms. Several biologically plausible routes connect vitamin D deficiency to ovarian dysfunction:
1) Reduced VDR signaling in ovarian tissue: Lower vitamin D availability may lessen VDR-mediated regulation of follicle development and steroid production.
2) Oxidative stress: Vitamin D may help moderate oxidative stress. When oxidative pressure rises, follicular health can suffer.
3) Inflammation modulation: Vitamin D influences immune pathways. Since chronic low-grade inflammation is common in ovarian disorders, deficiency may worsen inflammatory signaling.
4) Metabolic effects: Vitamin D may influence insulin sensitivity. Insulin dysregulation can contribute to hyperandrogenism, affecting ovulation and follicular growth.
These mechanisms don’t guarantee causation for each individual. Still, they create a coherent narrative for why vitamin D could be a meaningful piece of the puzzle—especially in recurrent or persistent ovarian issues.
Dietary Vitamin D, Sun Exposure, and Absorption Factors
Vitamin D status reflects both intake and biology. Some people can’t rely on sun exposure due to skin tone, latitude, climate, or lifestyle. Others may have absorption challenges due to gastrointestinal conditions, certain medications, or limited dietary diversity. Even with adequate exposure, vitamin D can vary widely based on body composition and metabolic factors.
Food sources include fatty fish, fortified dairy alternatives, egg yolks, and fortified foods. However, many diets still fall short. That’s why clinicians often evaluate vitamin D levels rather than guessing. When deficiency is present, correcting it—through diet, safe sunlight, or supplementation—may support broader reproductive health strategies.
Symptoms and Clinical Clues: When to Consider Testing
Vitamin D deficiency can be subtle. Some people experience fatigue, muscle aches, frequent infections, or low mood. Yet those symptoms overlap with many conditions, so they aren’t diagnostic. The more practical approach is context: if someone has irregular periods, symptoms suggestive of PCOS (such as acne, excess facial/body hair, or difficulty conceiving), recurrent ovarian cyst diagnoses, or metabolic concerns (like weight changes or insulin resistance), checking vitamin D may be reasonable.
Testing typically involves a blood measurement of 25-hydroxyvitamin D. Clinicians can then interpret results alongside other reproductive markers—such as hormones, glucose/insulin metrics, and pelvic ultrasound findings. This layered approach prevents the common trap of chasing a single nutrient as a standalone cure.
What the Evidence Suggests: Association, Not Instant Proof
Research often shows correlations between lower vitamin D levels and ovarian dysfunction patterns. But association isn’t identical to cause. A deficiency might contribute to susceptibility, or it might reflect lifestyle and metabolic factors that co-travel with ovarian problems. The body is rarely linear. Hormonal systems are dynamic, changing across time and influenced by stress, sleep, nutrition, and energy balance.
That said, a growing body of clinical discussions explores whether restoring vitamin D could improve cycle regularity, hormone profiles, and possibly inflammatory markers. Outcomes may be variable, depending on baseline vitamin D level, dose, adherence, and the underlying type of ovarian cyst issue.
Supplementation: Potential Benefits and Practical Cautions
For individuals with confirmed deficiency, supplementation is often considered. Vitamin D dosing should be personalized, and it’s wise to coordinate with a healthcare professional—particularly for people with kidney disease, granulomatous disorders, or those taking medications that influence calcium metabolism.
Why the caution? Excess vitamin D can raise calcium levels, potentially leading to complications. A thoughtful plan typically involves confirming the baseline level, choosing an appropriate dose, and rechecking levels after a period of time. It’s not simply “more is better.” It’s “enough to normalize signaling.”
Importantly, vitamin D support should be integrated with other evidence-informed strategies. For PCOS-related patterns, lifestyle measures targeting insulin sensitivity and inflammation can matter as much as any single supplement.
Beyond Vitamin D: The Broader Lifestyle and Hormone Landscape
Vitamin D exists in a network. Even if deficiency plays a role, ovarian cyst risk and recurrence are influenced by:
• Energy balance and metabolic health: Insulin resistance and weight changes can worsen ovulatory irregularity.
• Sleep and stress hormones: Chronic stress can affect reproductive signaling.
• Physical activity: Regular movement can improve metabolic parameters and inflammation.
• Nutrient sufficiency: Magnesium, omega-3 fats, and overall dietary quality can support hormonal resilience.
When these elements align, the ovarian environment becomes more stable. Vitamin D can then act as an amplifier rather than a solitary fix.
Meal Planning and “What to Avoid” Narratives Around Cysts
Nutrition conversations around ovarian cysts often include “what to avoid,” usually focusing on high glycemic foods, excessive refined sugars, and ultra-processed patterns that can aggravate insulin dynamics. While the details depend on the individual, the overarching logic is metabolic: smoother blood sugar control may support more consistent ovulation and reduce hormonal turbulence.
Instead of a restrictive mindset, aim for stabilizing habits—balanced meals with protein, fiber-rich carbohydrates, and healthy fats. Adequate micronutrients also matter. Vitamin D itself can’t be fully obtained through these foods in many cases, but diet can support the overall endocrine milieu.
Different Readers, Different Needs: How This Topic Can Help You
Not everyone reads about vitamin D and ovarian cysts for the same reason. Some readers are newly diagnosed with cysts and want practical next steps. Others have recurrent episodes and feel like they’re searching for a root cause. There are also readers managing PCOS who want to refine their approach beyond basics.
For practical readers, the value lies in questions to discuss with a clinician: vitamin D testing, other relevant labs, and whether supplementation could realistically help in their specific situation. For detail-oriented readers, the value lies in understanding mechanisms—VDR signaling, inflammation modulation, and metabolic coupling. For emotionally exhausted readers, the value lies in context: cyst patterns are multifactorial, and correcting deficiency is one potentially constructive step among several.
Whichever category fits, the narrative stays consistent—vitamin D may influence ovarian health, but it works best as part of an integrated plan.
The Takeaway: A Thoughtful Link Worth Investigating
The link between vitamin D and ovarian cyst patterns is compelling enough to deserve attention, especially when deficiency is present or ovarian dysfunction resembles PCOS. Vitamin D appears to influence ovarian microenvironment stability through immune modulation, oxidative stress control, and metabolic pathways that shape hormone balance.
Yet the most productive stance is not certainty—it’s clarity. Test when appropriate, interpret results within the full clinical picture, and pursue normalization alongside lifestyle and medical guidance. In that balanced framework, vitamin D can move from being a vague wellness idea to a concrete piece of reproductive health strategy.




