
Most people think of vitamin D as a simple “sunshine nutrient,” the kind you either have or you don’t. Yet the story is rarely that binary. Ask any clinician to interpret a vitamin D blood test and you’ll hear a familiar refrain: it depends on the cutoff being used, the lab’s measurement method, and the person sitting in front of them. Still, one question rises above the rest—what vitamin D level is too low? The answer is not only about numbers. It’s about thresholds, biology, and the surprisingly intricate ways your body negotiates calcium, immunity, and even cellular communication.
If you’ve ever stared at a lab report—something like “25(OH)D”—and felt a slight chill at the uncertainty, you’re not alone. The fascination comes from a deeper truth: vitamin D is both a nutrient and a hormone-like regulator. When it dips, the symptoms can be subtle at first, then insistently louder, like a distant alarm turning into a steady hum.
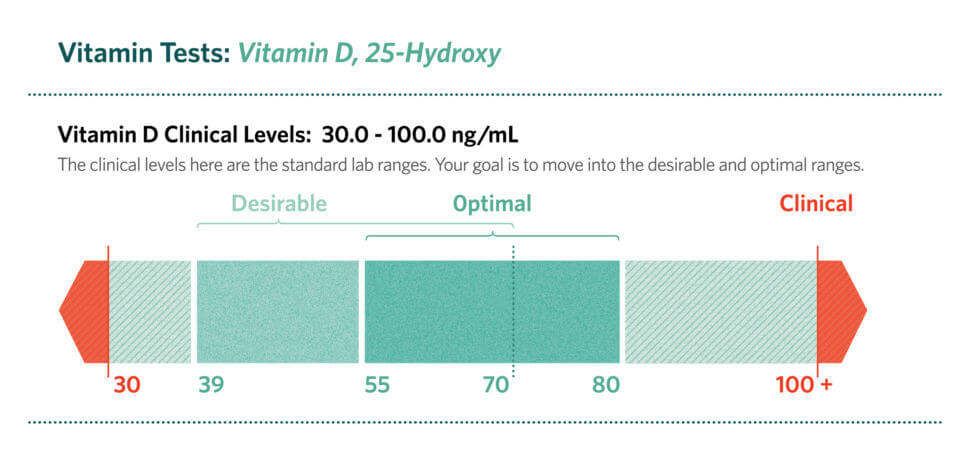
Understanding the Test: What “25(OH)D” Really Means
The vitamin D most commonly measured is 25-hydroxyvitamin D, written as 25(OH)D. This marker is popular because it reflects your body’s vitamin D stores more reliably than the more transient active forms. In everyday terms, it’s the “inventory” signal.
Why does this matter for deficiency ranges? Because vitamin D status is not just about what you ate yesterday or what your skin made last week. It’s about accumulation, conversion, and utilization. Some people build stores efficiently; others leak them away through lifestyle factors, metabolic quirks, or medical conditions.

The Central Question: When Does Vitamin D Become “Too Low”?
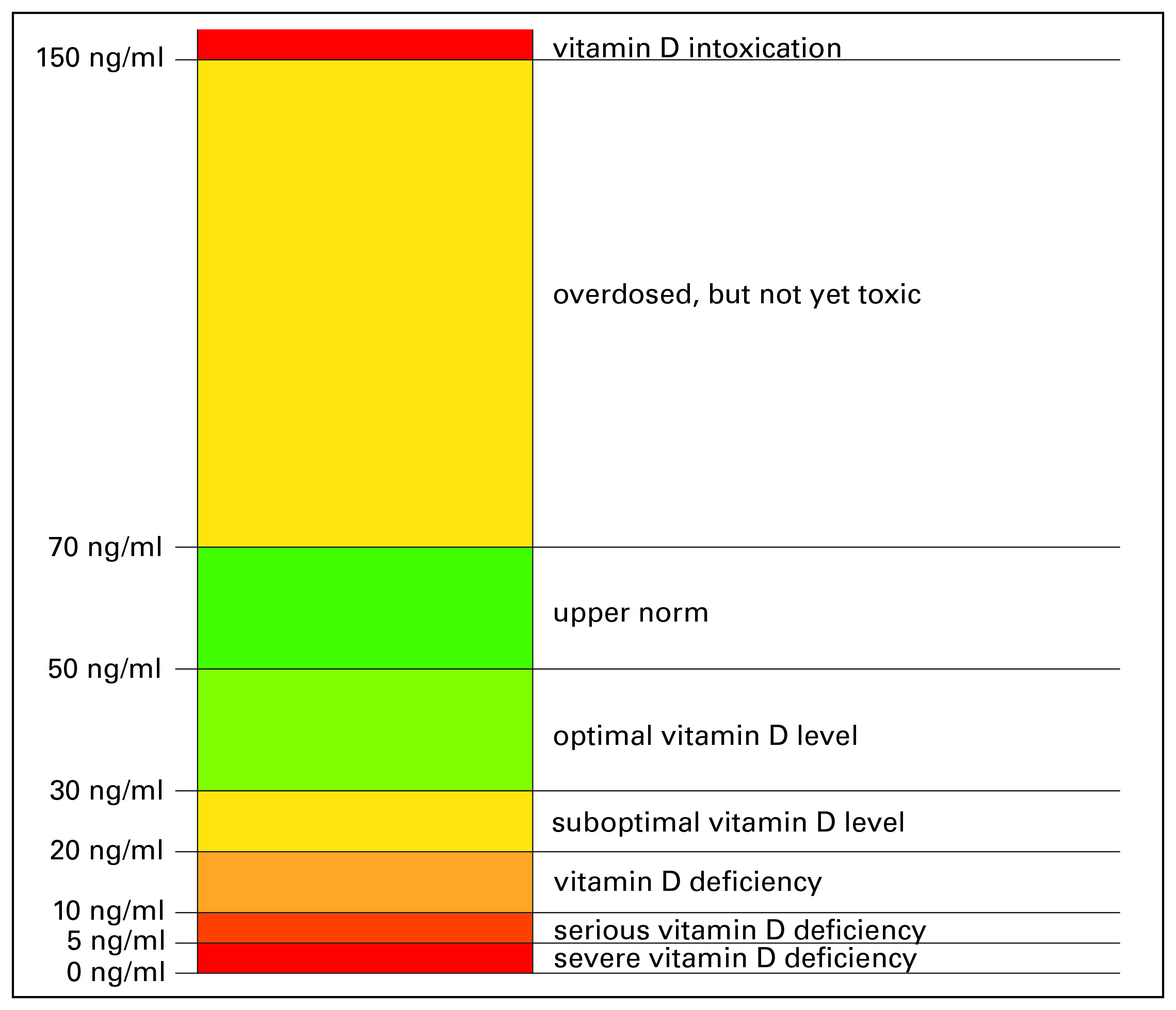
Deficiency ranges vary slightly between guidelines, but the structure is remarkably consistent. Most clinical frameworks place low vitamin D into tiers—deficient, insufficient, or adequate—based on the concentration of 25(OH)D in the blood.
In many widely used interpretations:
• Below ~20 ng/mL (50 nmol/L): commonly treated as insufficient or deficient depending on the system.
• Below ~12–15 ng/mL (30–37.5 nmol/L): often classified as deficiency in stricter definitions.
• Above ~20–30 ng/mL (50–75 nmol/L): frequently considered adequate, though some experts target higher values for specific outcomes.
Here’s the twist: “too low” isn’t just a scientific label. It’s a physiological pressure point. Below certain thresholds, the body’s ability to maintain calcium balance and support bone mineralization starts to wobble. Over time, that wobble can become a strain.
Deficiency vs. Insufficiency: The Gray Zone That Feeds Confusion
One of the most common observations is that different websites—and sometimes different doctors—give slightly different answers for the same blood number. This is why the words deficient and insufficient are so important. They are not merely semantic. They represent different clinical attitudes about risk.
In the borderline range, many individuals show no obvious symptoms. That absence of warning signs is itself a form of misdirection. Vitamin D-related changes can progress silently: subtle muscle weakness, fatigue, or a gradual shift in immune tone. Then, once another factor—an illness, reduced mobility, pregnancy, or aging—enters the stage, the imbalance becomes more visible.
So the “gray zone” is fascinating because it behaves like a dimmer switch rather than an on/off switch. Your body may compensate for a while, but compensation costs energy.
How Low Vitamin D Can Echo Through the Body
Vitamin D’s most famous job is supporting bone health. When vitamin D is too low, the gut absorbs less calcium. The result can be secondary changes in parathyroid hormone (PTH), which works to protect blood calcium levels by pulling from bone stores. Over time, this can contribute to bone thinning and an increased risk of fractures.
But bones aren’t the only audience. Vitamin D interacts with immune signaling pathways, influencing how the body calibrates inflammation and immune responses. Some research associations link low vitamin D with higher susceptibility to certain conditions, including some cancers and metabolic disorders. These relationships do not always prove direct causation, yet they do suggest that vitamin D may act like a biological “conductor,” shaping how multiple systems coordinate.
In other words: low vitamin D can be a symptom of something broader—and sometimes the cause, too.
Who Is Most Likely to Have Low Vitamin D?
It’s tempting to assume low vitamin D happens only to people who avoid sunlight. Sun exposure matters, but it’s not the only lever. Many factors act together like overlapping gears.
Common risk categories include:
• People living at higher latitudes or with limited outdoor time.
• Individuals with darker skin, where melanin reduces vitamin D synthesis efficiency.
• Older adults, whose skin can synthesize vitamin D less effectively.
• People who consistently wear clothing that limits skin exposure.
• Those with obesity, since vitamin D can become sequestered in adipose tissue.
• Individuals with malabsorption issues (such as celiac disease, Crohn’s disease, or pancreatic insufficiency).
• People taking certain medications that affect vitamin D metabolism.
Notice how many of these categories are really about conversion, absorption, or storage. That hints at a deeper reason for fascination: vitamin D status is often an indirect portrait of broader physiology.
The Deep Reason It’s Hard to Pin Down: Measurement, Metabolism, and Individual Variation
Even with the same “25(OH)D” value, people can experience different effects. Why? Because vitamin D operates within a metabolic ecosystem. Your body must absorb it through the gut (when consumed), convert it in the liver, and then activate it in the kidneys. Hormones like PTH, differences in vitamin D binding proteins, and varying degrees of inflammation all shape the outcome.
Additionally, lab methods and reference ranges can differ. That means one lab’s “low” might correspond to another lab’s “borderline.” The number alone rarely tells the whole story.
Consider this a subtle lesson: your lab result is a snapshot. Your physiology is a moving film.
Symptoms and Signs: What Low Vitamin D Can Look Like
Low vitamin D doesn’t always announce itself with dramatic symptoms. Often, the first signs are ordinary—so ordinary they’re easily ignored.
Possible clues include:
• Muscle weakness or aching, especially in the thighs and hips.
• Fatigue that feels chronic rather than seasonal.
• Bone discomfort or increased risk of fractures over time.
• Mood changes in some individuals, though the evidence varies by study.
If deficiency is significant, certain populations—particularly older adults—may experience faster functional decline. That’s why some clinicians treat low vitamin D not as a cosmetic issue, but as a lever affecting mobility and resilience.
How Clinicians Respond: Retesting, Targeting, and Supplementation Logic
Once a vitamin D level is identified as too low, the next step is rarely “one-size-fits-all.” Clinicians consider severity, symptoms, dietary intake, sunlight exposure, and risk factors for absorption problems.
Common strategies include supplementation with vitamin D3 (cholecalciferol) or sometimes D2 (ergocalciferol). Dose selection often aims to raise levels gradually and maintain them afterward. Retesting is typically recommended to confirm response and avoid persistent under-treatment—or overshooting.
It’s also helpful to consider co-factors. Calcium intake matters for bone health, while magnesium can influence vitamin D metabolism. Without the supporting cast, vitamin D supplementation may feel like adding fuel to a stove that lacks airflow.
So, What Is Too Low? A Practical Summary
If you want a clean answer to the question “What vitamin D level is too low?”, think in tiers:
• Mild insufficiency: roughly below ~20 ng/mL (50 nmol/L).
• More concerning deficiency: often below ~12–15 ng/mL (30–37.5 nmol/L), depending on guideline intensity.
• Generally adequate range: commonly around ~20–30 ng/mL (50–75 nmol/L), with some clinicians targeting higher values for specific contexts.
But the most important takeaway is this: the “right” interpretation depends on your health landscape—your age, absorption capacity, lifestyle, and the purpose behind the testing. Vitamin D is not merely a number. It’s a signal of how your body turns sunlight and food into usable regulation.
When vitamin D is too low, the fascination is justified: you’re not just chasing an optimal lab value—you’re decoding a biological story written across bone, immune signaling, and metabolism. And once you understand the story, the ranges stop feeling arbitrary and start feeling like navigation.





