
Osteoporosis rarely announces itself. It creeps in like a quiet draft—until a fracture makes the reality undeniable. For many women, the missing thread in that story is vitamin D. This nutrient—part hormone, part dietary “fuel”—helps the body turn calcium into something structural: resilient bone. When vitamin D is insufficient, the scaffolding of the skeleton becomes less trustworthy. And because osteoporosis is often silent, understanding the vitamin D connection can feel like discovering the hidden mechanism behind a problem you were already living with.
Bone Architecture: Why Osteoporosis Develops in the First Place
Bone is not inert tissue. It’s a living, constantly remodeling matrix where osteoclasts remove old material and osteoblasts rebuild. With age—especially after menopause—this cycle can tip toward net bone loss. Estrogen withdrawal accelerates remodeling, and the balance of mineralization becomes harder to maintain.
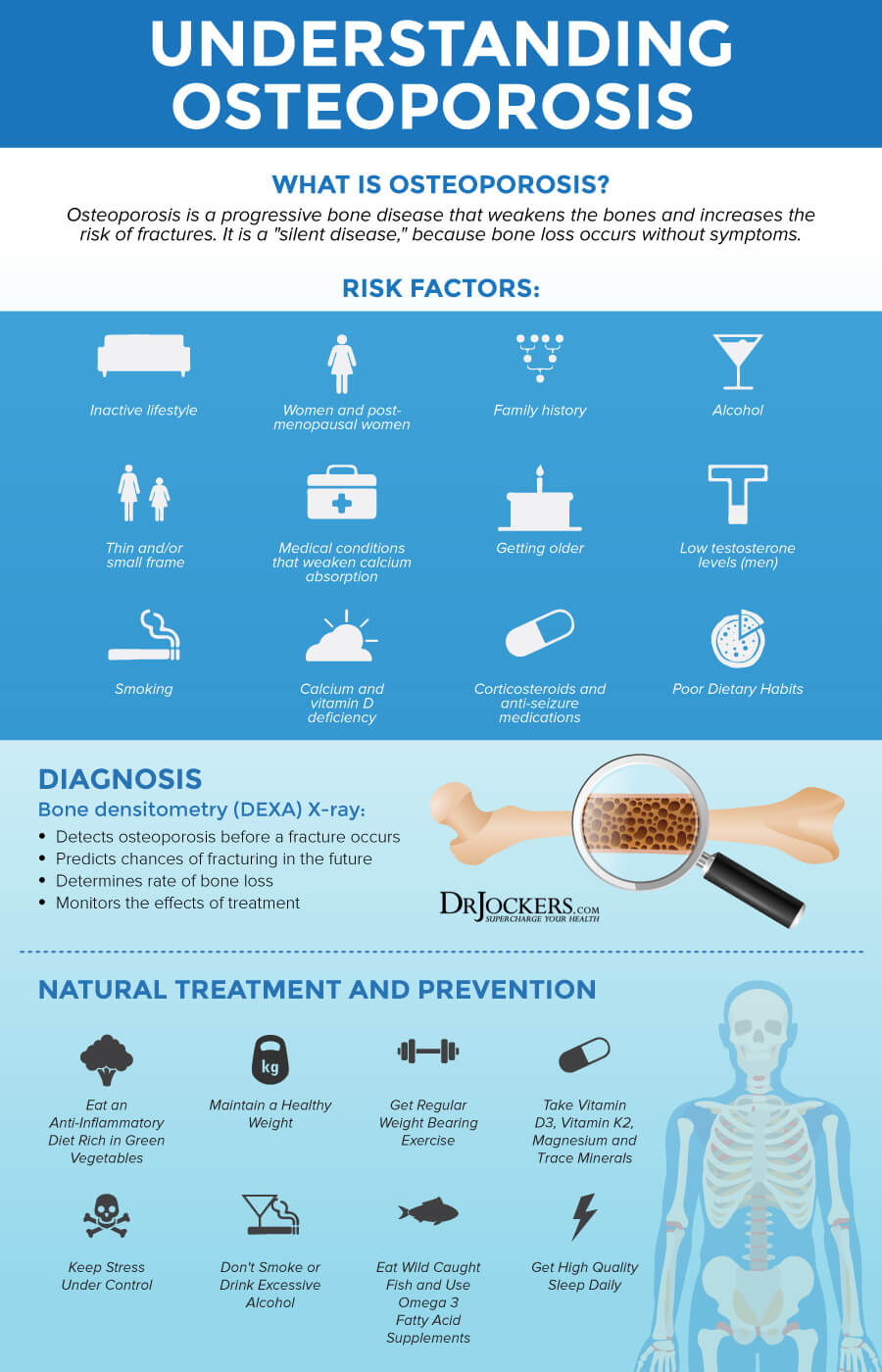
Osteoporosis is defined not merely by “thin bones,” but by weakened microarchitecture: the internal lattice becomes porous, and fractures become more likely even after minor falls. What makes this condition especially concerning for women is that risk often increases steeply during the postmenopausal years.
Within this remodeling process, mineralization is crucial. Calcium must be deposited at the right time and in the right configuration. Vitamin D is a gatekeeper for that process, quietly influencing how effectively the body absorbs and uses calcium.
Vitamin D at the Cellular Level: The Hormone Behind Calcium Absorption
Vitamin D is remarkable because it functions like a hormone. After activation in the liver and kidneys, it influences gene expression in the gut, enabling more efficient calcium absorption. In practical terms, adequate vitamin D helps ensure that dietary calcium doesn’t pass through unused—it gets carried into the bloodstream and delivered to bone.
When vitamin D is low, calcium absorption can drop. The body may compensate by pulling calcium from bone, which is not an emergency response anyone wants to rely on long-term. This is one reason chronic deficiency may contribute to bone fragility.
It’s also why vitamin D is often described as an “indirect builder.” It doesn’t replace calcium, nor does it magically rebuild lost bone. Instead, it supports the biochemical conditions necessary for bone to mineralize properly.

How Low Vitamin D Becomes a Quiet Risk Amplifier
Low vitamin D rarely causes dramatic symptoms. Fatigue can occur, but it’s nonspecific and easy to ignore. Meanwhile, bone health can steadily decline. This delay creates a deceptive comfort: people often feel fine while their skeleton loses mineral density.
Several factors can raise the odds of vitamin D deficiency. Limited sun exposure is the most common culprit. Sunscreen use can reduce skin synthesis, although it doesn’t eliminate it completely. Higher latitude, winter seasons, indoor lifestyles, darker skin pigmentation, and aging skin all reduce the body’s efficiency at producing vitamin D.
Diet matters too. Many women don’t consistently consume vitamin D–rich foods, and some have difficulty absorbing nutrients due to gastrointestinal conditions or certain medications.
Who Is Most Likely to Be Affected: Risk Profiles for Women
Osteoporosis risk is not uniform. Age is a powerful variable, but it’s not the only one. Postmenopausal women are particularly vulnerable, especially those with early menopause, a history of prolonged estrogen deficiency, or a family history of fragility fractures.
Some medical circumstances also elevate risk. Chronic kidney disease can disrupt vitamin D activation. Malabsorption syndromes can reduce absorption of vitamin D and calcium simultaneously. Thyroid disorders, certain anticonvulsants, and long-term corticosteroid therapy can increase bone loss while also complicating vitamin D metabolism.
Then there are lifestyle factors: smoking, excessive alcohol consumption, low body weight, and limited weight-bearing activity all interact with mineral metabolism. Think of them as additional moving parts—when vitamin D is already low, the entire system becomes more unstable.
Symptoms You Should Not Ignore: From Subtle Clues to Fracture Alarms
Because osteoporosis is frequently asymptomatic, the most important “symptom” is often absence of warning. Still, some signs deserve attention. Loss of height, a stooped posture, or back pain may reflect vertebral compression fractures—injuries that can be missed until they accumulate.
New fractures after minimal trauma—such as a fall from standing height—should be treated as a red flag, not a coincidence. In these moments, vitamin D status often becomes part of the diagnostic conversation, because fracture risk can be influenced by inadequate mineralization.
Early recognition matters. The sooner osteoporosis is identified, the more effectively treatment can slow progression and reduce the likelihood of further injury.
Testing for Vitamin D and Bone Health: What to Expect
Understanding the vitamin D connection usually begins with measurement. Clinicians often use a blood test to check vitamin D levels (commonly 25-hydroxyvitamin D). Interpretation can vary by laboratory standards and clinical guidelines, but the general goal is to identify whether deficiency or insufficiency is present.
Bone density testing (like a DEXA scan) evaluates mineral density and helps estimate fracture risk. A DEXA scan doesn’t diagnose vitamin D deficiency directly, but it can reveal whether bone loss is already underway.
Sometimes additional labs are considered, including calcium, phosphorus, parathyroid hormone, and markers related to bone turnover. The idea is to understand the metabolic environment surrounding bone remodeling.
Diet, Sunlight, and Supplementation: Building a Practical Strategy
Vitamin D can come from sunlight exposure, diet, and supplements. Sunlight is efficient, but it’s not always dependable. Weather, latitude, and lifestyle patterns can reduce consistent synthesis. Many women also prefer predictable, controlled approaches rather than relying solely on sun.
Dietary sources include fatty fish (like salmon and sardines), fortified dairy products, fortified plant milks, egg yolks, and fortified cereals. However, dietary vitamin D alone may not be enough for everyone—especially when deficiency is already established.
Supplementation can help close the gap, but dosing should be individualized. Too little may be ineffective; too much can be harmful. A clinician-guided plan is especially important when there are kidney issues, hypercalcemia concerns, or complex medication regimens.
Calcium intake often pairs with vitamin D strategies. Bones need both mineral supply and the hormonal assistance that ensures the mineral gets used.

Vitamin D and Osteoporosis Treatments: How the Pieces Fit Together
Vitamin D is not a standalone cure for osteoporosis. Osteoporosis treatment typically involves a combination of lifestyle measures, fall prevention, and medication when risk is high. Pharmacologic options may include antiresorptive agents or bone-building therapies, depending on the individual scenario.
That said, vitamin D often functions as a foundational support. If someone begins osteoporosis treatment while vitamin D is severely low, the body may struggle to handle mineralization demands effectively. Correcting deficiency can improve outcomes and reduce the chance of complications related to calcium metabolism.
It’s a synergy concept: medications may change remodeling dynamics, while vitamin D and calcium help ensure the raw materials and biochemical environment support new bone integrity.
Lifestyle Interventions: Weight-Bearing Movement and Bone-Friendly Habits
Even with vitamin D optimization, bone health needs mechanical stimulus. Weight-bearing exercises—like brisk walking, stair climbing, dancing, or low-impact aerobics—encourage bone to maintain density. Resistance training adds a further advantage by strengthening muscles that protect the skeleton during falls.
Balance work is quietly crucial. The most sophisticated treatment can’t prevent fractures if falls are frequent. Simple interventions—vision checks, home hazard removal, appropriate footwear—can be as bone-protective as a supplement bottle.
Nutrition also extends beyond vitamin D. Adequate protein supports collagen structures, while fruits and vegetables provide micronutrients that support overall tissue health. Bone is not only mineral—it’s an engineered framework with organic components.
Common Misconceptions: What Women Often Get Wrong
One misconception is that vitamin D is only relevant for sun worshippers or people who never go outdoors. Modern life can be indoors by default, and even regular outdoor time may not ensure sufficient synthesis—especially in older skin.
Another myth is that vitamin D “rebuilds bones” quickly. Bone remodeling is slow by design. Vitamin D supports the environment for mineralization, but osteoporosis treatment and fracture risk reduction require sustained, multi-layered efforts.
Finally, some assume that because vitamin D can be measured in blood, it guarantees bone safety. Bone density depends on many inputs—hormones, genetics, activity, nutrition, medications, and aging. Vitamin D is important, but it’s part of a larger ecosystem.
Taking Action: A Personalized, Evidence-Aware Next Step
If osteoporosis risk feels like a looming possibility, it’s reasonable to act early rather than waiting for a fracture to confirm the threat. Start with assessing risk factors. Then consider asking about vitamin D testing and bone density evaluation if appropriate.
Pair any vitamin D plan with practical nutrition, sensible supplementation (when needed), weight-bearing exercise, and fall prevention measures. The goal is not simply to raise a lab number—it’s to strengthen bone quality and reduce vulnerability in everyday life.
When the osteoporosis-vitamined connection is understood, prevention becomes more than a slogan. It becomes a coordinated strategy: biochemical support, mechanical strength, and protective habits working together. That’s how women turn uncertainty into control—one measured, sustained step at a time.




