Vitamin D has long carried a curious double life: part sunshine’s messenger, part molecular locksmith, turning cellular “locks” just enough to open doors that the immune system can then walk through. When tuberculosis (TB) enters the narrative, the story becomes even more compelling. TB is an ancient adversary, resilient and patient—like a smoke-filled hallway that waits for the lights to flicker. Vitamin D, in contrast, behaves like a small lantern held near the wall: it cannot erase the entire darkness, but it can change what the immune cells notice, and how effectively they respond. The question “Vitamin D for tuberculosis?” is therefore not merely pharmacologic. It is historical, mechanistic, and deeply human—an ongoing attempt to understand whether a nutrient shaped by sunlight can also tune the body’s defenses against a microbe that prefers the shadows.
From folklore to lab bench: an unexpected historical thread
Long before randomized trials quantified outcomes, clinicians observed patterns. TB seemed to flourish in places where sunlight was scarce, and in eras when indoor living and soot-blackened skies were common. People noticed that fresh air and light had a kind of restorative gravitas. In that older clinical imagination, vitamin D was not yet a named substance—yet its physiological footprint was implicitly present. The leap from “light helps” to “vitamin D mediates protection” required scientific translation: separating correlation from mechanism, and hope from biology.
As the twentieth century unfolded, researchers clarified how vitamin D is synthesized and metabolized. Sunlight becomes a precursor; the liver and kidney process it into active forms. In the immune system, this is not a trivial detour. It is akin to giving defensive cells a set of adjustable knobs. Rather than simply “boosting immunity” in a vague sense, vitamin D appears to influence immune signaling pathways that govern how macrophages respond to intruders.
And TB, with its slow-burn strategy inside macrophages, becomes the perfect stage. TB does not merely invade tissue; it co-opts cellular machinery. So if vitamin D can modify macrophage behavior, it might plausibly alter the course of TB infection or disease progression.
The vitamin D–immune axis: how the lantern becomes a toolkit
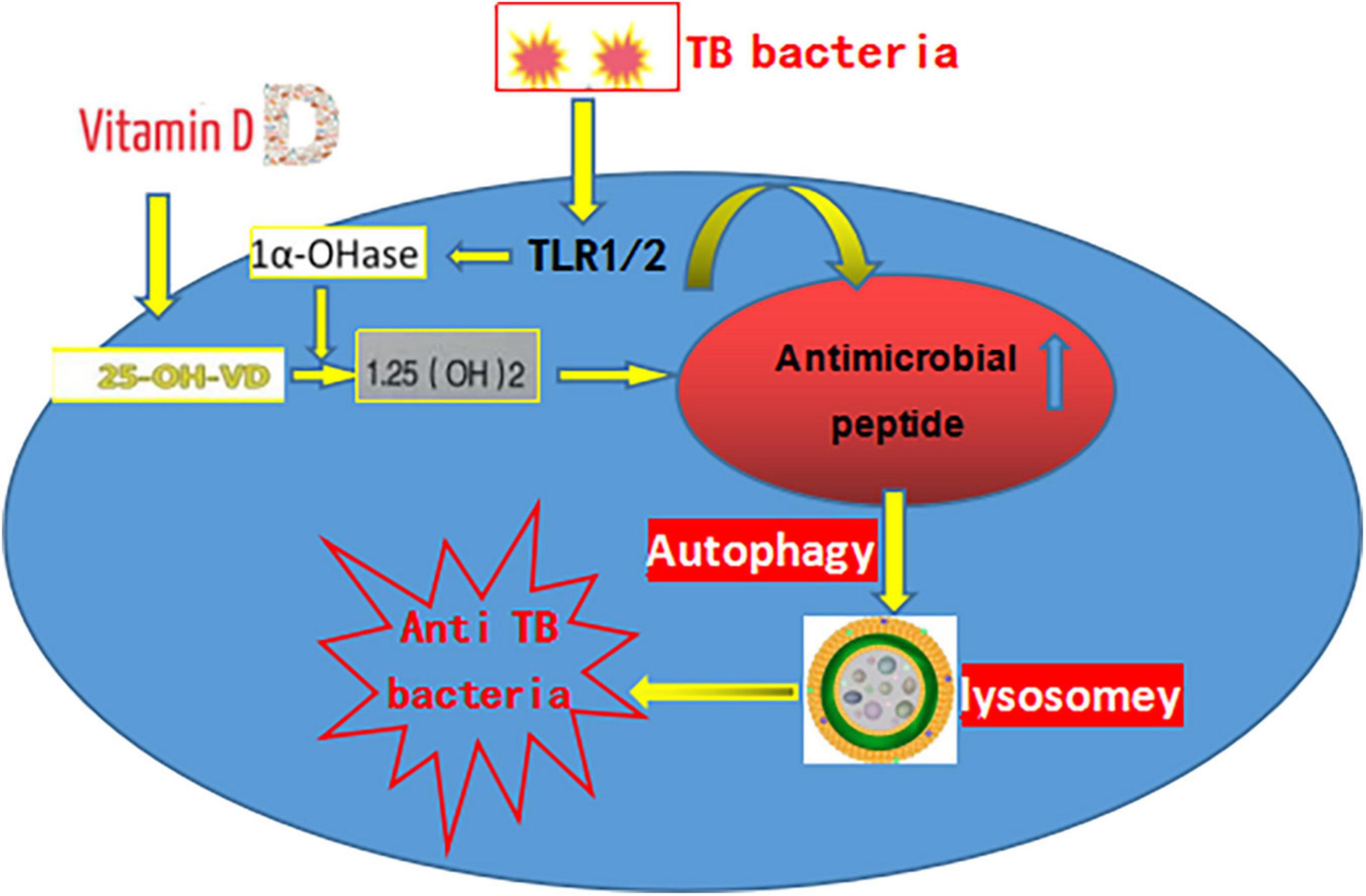
Mechanistically, vitamin D’s appeal lies in its ability to reshape gene expression in immune cells. Active vitamin D interacts with the vitamin D receptor (VDR), which functions like a transcriptional switch. When macrophages and other immune cells receive the signal, they may increase production of antimicrobial peptides. These peptides behave like molecular “spears,” aimed at constraining microbial survival.
Vitamin D also influences other immune dynamics. It can modulate inflammatory signaling, potentially steering the immune response away from harmful excess while preserving effective containment. This balance is crucial. TB pathology is not only driven by the bacterium; it is also fueled by the immune system’s collateral activity. A molecule that adjusts intensity—rather than just inflating it—may therefore be uniquely valuable.
There is also a more nuanced concept: the body’s defense readiness. Vitamin D status can affect how quickly immune cells mount effective responses. Think of it as winter gear stored in a closet: when the cold arrives, timing matters. Adequate vitamin D might mean the immune system is not fumbling for thermal protection when TB is trying to settle in.
What “deficiency” changes in TB risk and severity
Vitamin D deficiency is common in many populations and is intensified by limited sun exposure, darker skin pigmentation, aging, obesity, and certain dietary patterns. In TB, these risk factors can overlap with socioeconomic conditions that influence nutrition, access to healthcare, and exposure risk. This creates a complex tapestry. Low vitamin D might be both a marker of broader vulnerability and a contributor to impaired immune performance.
Observational studies have frequently associated lower vitamin D levels with higher TB susceptibility, and with differences in disease severity or treatment response. However, associations can be treacherous. They may reflect confounding variables such as nutritional insufficiency, comorbidities, or baseline inflammatory states that alter vitamin D metabolism.
Even so, the biological plausibility remains. If vitamin D modifies macrophage competence and antimicrobial signaling, deficiency could plausibly weaken the early containment of TB—allowing the bacterium more time to establish a strong foothold.
Sunlight, seasonality, and the puzzle of exposure
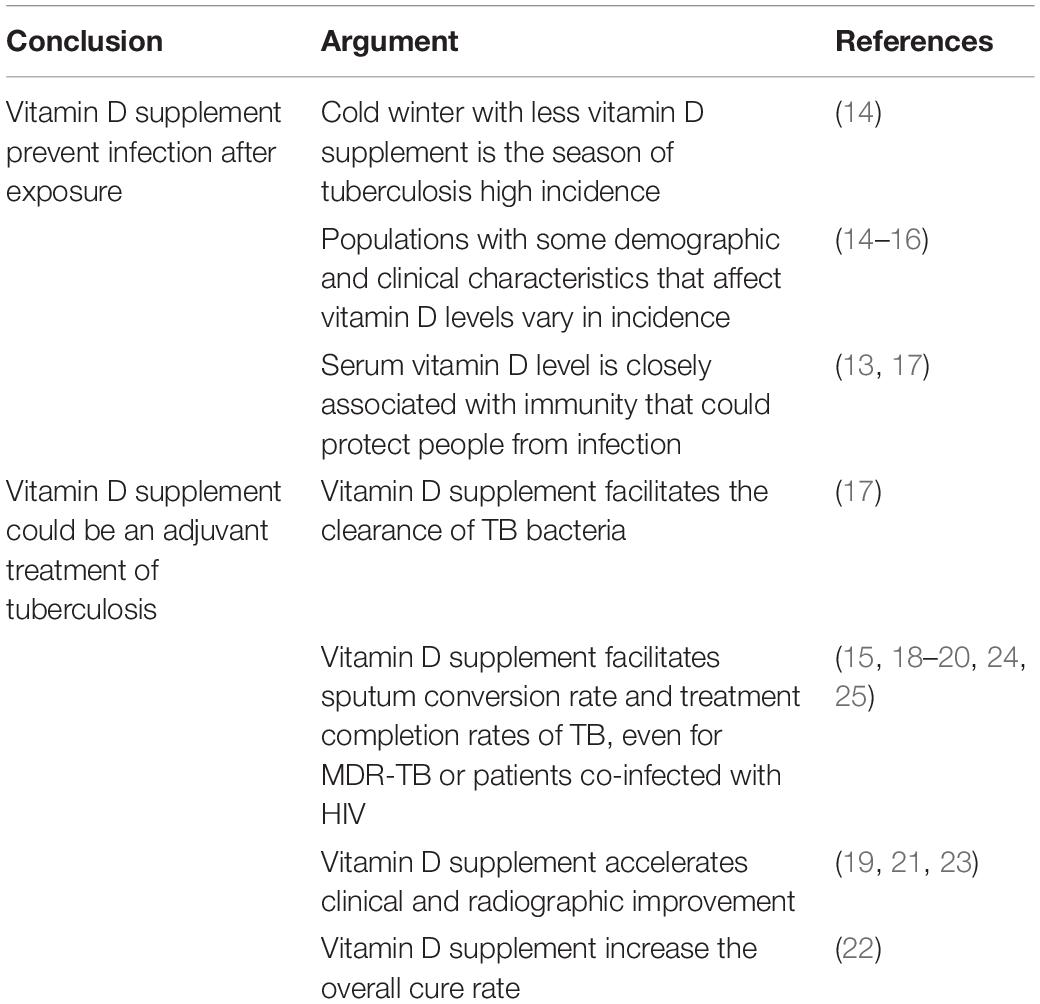
Because vitamin D is synthesized through ultraviolet exposure, seasonal rhythms become relevant. TB incidence can vary by climate and geography, and sunlight patterns can influence vitamin D levels across the year. This invites a fascinating hypothesis: when sunlight rises, vitamin D availability improves, and immune conditions may become more favorable against TB.
Yet nature rarely cooperates with simple timelines. TB infection can occur long before symptoms declare themselves. Latency is a hidden calendar, and disease onset may lag behind seasonal shifts. Therefore, even if vitamin D exerts influence, the measurable epidemiologic relationship may be delayed, blurred, or counterbalanced by other seasonal factors—crowding patterns, respiratory virus circulation, and variations in healthcare access.
Still, seasonality strengthens the idea that vitamin D might be more than an isolated nutrient. It may represent an ecological signal of immune readiness influenced by environment.
Drug-adjunct hopes: what clinical trials have attempted
Modern clinical research has tested vitamin D as an adjunct to standard TB therapy. The ambition is clear: could supplementation improve sputum conversion, reduce time to culture negativity, lower relapse rates, or influence overall mortality? If vitamin D helps immune cells coordinate effective antimicrobial activity, it might accelerate disease control.
Trial results, however, have not been uniformly triumphant. Some studies suggest potential benefits in certain subgroups, while others show minimal or no effect. This inconsistency is not merely disappointing—it is informative. TB is heterogeneous. Participants vary by baseline vitamin D status, bacterial burden, HIV status, nutritional patterns, adherence, and genetic differences affecting vitamin D receptor pathways.
When outcomes fail to align across trials, the underlying message often points to effect modification: vitamin D might not be a universal lever. Instead, it may operate like a key that fits certain locks. Those with profound deficiency might gain more. Those with adequate levels may experience little additional benefit.
There is also the dosing question. “More” is not automatically “better.” Excessive dosing can carry risks, and the immune system’s response may follow a bell-shaped curve—too little fails, optimal helps, too much may become counterproductive or physiologically disruptive.
Heterogeneity and genetics: why “one dose fits all” rarely survives biology
TB research repeatedly demonstrates that biology refuses to be averaged. Vitamin D’s effects depend on receptor expression and downstream signaling. Genetic polymorphisms in the VDR gene and in enzymes involved in vitamin D metabolism can alter responsiveness. Some individuals may translate vitamin D into stronger antimicrobial signals; others may receive only a weak cellular echo.
Furthermore, TB co-infections and comorbidities can reshape the immune landscape. HIV, for instance, profoundly affects immune function and can alter vitamin D metabolism. Diabetes, chronic kidney disease, and malabsorption disorders can complicate the relationship between supplementation and active vitamin D availability.
Therefore, a nuanced view emerges: vitamin D may be most helpful where it is missing, where immune pathways are intact enough to respond, and where supplementation can meaningfully correct a deficit rather than simply add surplus.
Immunology as metaphor: a rehearsal, not a miracle
Consider TB as an accomplished improviser. It thrives on timing—waiting for macrophages to falter, for inflammatory noise to become confused, and for containment to loosen. Vitamin D, in this metaphor, is not a superhero arriving with a cape. It is a rehearsal director. It helps immune cells practice the choreography before the performance begins.
In some contexts, the rehearsal improves the outcome dramatically. In others, the rehearsal schedule is irrelevant because the theater is poorly equipped, the cast is missing, or the script has already diverged. That is why clinical results vary. Vitamin D’s impact depends on whether the immune system can actually benefit from the rehearsed instructions.
This metaphor also clarifies why absence of universal effectiveness does not invalidate mechanistic promise. A rehearsal can be transformative—when it happens at the right moment, for the right ensemble.
Public health and practical guidance: where supplementation may matter most
From a public health perspective, vitamin D supplementation may be most compelling as part of broader nutritional strategy rather than as a stand-alone TB intervention. Ensuring adequate nutrition, addressing malnutrition, promoting safe sunlight exposure where feasible, and correcting vitamin D deficiency could support overall resilience.
For clinicians, the key is discernment: identifying patients at higher risk of deficiency, considering baseline levels when available, and balancing potential benefit against dosing safety. For some individuals, optimizing vitamin D status could plausibly improve immune readiness during TB treatment. For others, the effect may be negligible.
In high-burden settings, logistical realities matter. Supplementation programs should be integrated thoughtfully into existing TB care pathways rather than treated as an isolated experiment.
Looking forward: biomarker-driven strategies and precision questions
The next wave of research likely needs sharper tools. Baseline vitamin D status, genetic markers, immune profiling, and treatment response phenotyping could help determine who benefits most. Instead of asking whether vitamin D helps TB in general, future studies can ask targeted questions: does it help the severely deficient? does it shorten time to microbiologic cure in specific populations? does it reduce relapse under particular immunologic conditions?
Biomarkers could transform uncertainty into clarity. If specific immune signatures predict response to vitamin D, supplementation could become a precision adjunct. This would honor the unique appeal of vitamin D: not that it is universally powerful, but that it may be exquisitely conditional—powerful where it is needed.
The scientific horizon is therefore both cautious and hopeful. TB is formidable, but so is methodical inquiry. Vitamin D remains a fascinating candidate in the immune choreography—waiting for the right conditions to prove its most useful role.
Conclusion: a conditional lantern in the TB landscape
Vitamin D and tuberculosis form a relationship that is neither purely myth nor fully resolved medicine. Historically, light and wellbeing were linked in the public imagination. Scientifically, vitamin D’s immune modulation offers plausible mechanistic pathways. Yet clinical evidence remains heterogeneous, suggesting vitamin D is not a universal cure, but a conditional modifier—most likely to matter when deficiency is present, when immune pathways can respond, and when dosing aligns with biology.
In the end, vitamin D’s intrigue lies in its dual identity. It is both environment-shaped and cell-directed. It hints that TB control is not only about attacking bacteria, but also about tuning the host’s internal landscape. A lantern cannot extinguish the night by itself, but it can change where threats are seen—and how quickly defenders move.




