
Gestational hypertension can arrive quietly—then suddenly make itself known in the second half of pregnancy. If you’ve been monitoring your blood pressure and wondering whether nutrition can meaningfully support your health, vitamin D often becomes part of the conversation. Not as a standalone “cure,” but as a potential contributor to cardiovascular stability, immune modulation, and vascular function during pregnancy. Let’s explore what vitamin D is believed to influence, what types of evidence and guidance readers can expect, and how practical decisions about testing and supplementation may fit into a safer, more informed prenatal routine.
Gestational Hypertension: What It Means for Moms and Babies
Gestational hypertension is characterized by new-onset elevated blood pressure after 20 weeks of pregnancy, typically without the specific markers that define preeclampsia. The distinction matters, because it shapes monitoring intensity and risk management. Short sentences can be reassuring: blood pressure is not just a number—it’s a pressure system that affects placental circulation, oxygen delivery, and overall maternal wellbeing.
In everyday terms, higher pressure can strain the delicate vascular network that sustains pregnancy. When blood vessels become less responsive, the placenta may receive blood less efficiently. That inefficiency can contribute to complications, so clinicians frequently track trends, symptoms, and lab indicators. Readers generally expect this section to clarify terminology, explain why timing and thresholds matter, and show how gestational hypertension differs from chronic hypertension and preeclampsia.
Where Vitamin D Fits: A Hormone with Vascular Consequences
Vitamin D is often described as a vitamin, but it behaves more like a hormone—synthesized in the skin, processed in the liver and kidneys, and then used throughout the body. Its influence extends beyond bone metabolism. It also participates in endothelial function, inflammatory signaling, and calcium regulation—processes that can affect blood pressure regulation.
Many readers find it helpful when vitamin D is framed through “systems thinking.” It’s not only about immune health or bone strength; it’s also about how blood vessels behave under stress. When vitamin D pathways are insufficient, some studies suggest the body may produce a more pro-inflammatory environment and impair vascular relaxation. This is where the narrative often shifts from simple supplementation to a more nuanced question: could adequate vitamin D help the body maintain calmer vascular tone during pregnancy?
The Mechanisms: Endothelial Function, Inflammation, and Renin–Angiotensin Signaling
Blood pressure regulation is complex, and vitamin D is thought to interact with multiple pathways. One major concept is endothelial function—the endothelium being the inner lining of blood vessels. If endothelial function is compromised, vessels may not dilate properly, and vascular resistance can increase.
Another frequently discussed theme is inflammation. Pregnancy already involves immune modulation, but when inflammatory signaling becomes disproportionate, vascular dysfunction may follow. Vitamin D is believed to influence immune behavior, potentially encouraging a more balanced inflammatory profile.
Renin–angiotensin pathways also appear in the conversation. These pathways help control blood vessel constriction and fluid balance. Some evidence suggests vitamin D may regulate components of this system, indirectly affecting blood pressure. Short and long sentences can coexist here: the logic is intricate, yet the goal is straightforward—more stable vascular regulation.
What Research Suggests: Associations, Mixed Findings, and Practical Interpretation
Readers deserve a realistic overview rather than a simplistic promise. Studies on vitamin D and gestational hypertension often include observational research and, in some cases, clinical trials. Observational studies can reveal patterns—such as whether low vitamin D status tends to appear more often among individuals with hypertension. But association is not the same as causation, and pregnancy introduces many confounders.
Clinical trials may produce mixed results depending on baseline vitamin D levels, dosing strategies, timing, adherence, and differences in population risk. This is where readers typically want clarity: “Should I take vitamin D?” and “Will it lower my blood pressure?” The most balanced interpretation is usually that correcting deficiency might support overall maternal health, while the blood pressure effect—if present—may be modest and not guaranteed.
To help readers navigate complexity, this section is commonly formatted with digestible subpoints: what the data tends to show, where it’s uncertain, and why individual factors matter.
Vitamin D Status: How Deficiency Is Identified During Pregnancy
Before supplementation becomes a guesswork exercise, many clinicians recommend checking vitamin D status via a 25-hydroxyvitamin D blood test. This marker reflects the body’s vitamin D stores more reliably than other forms. A reader-friendly approach includes explaining what “deficiency” and “insufficiency” commonly mean in clinical terms, while acknowledging that lab thresholds and guidelines can vary.
Low sun exposure, darker skin pigmentation, higher body mass index, limited dietary intake, and geographic latitude may all contribute to insufficient vitamin D levels. If you’re looking for a cohesive narrative, this section often connects lifestyle patterns to measurable lab outcomes.
It’s also useful to highlight that pregnancy changes physiology—so a level that was acceptable pre-pregnancy may not remain optimal as gestation progresses. Long sentences can help: nutrition doesn’t exist in isolation; it’s carried through the changing physiology of pregnancy.
Dietary Sources and Sunlight: Supportive, Not Always Sufficient
Diet can contribute to vitamin D intake, but it frequently falls short—especially during late pregnancy or in regions with limited sunlight. Fatty fish (like salmon and sardines), fortified dairy or plant milks, fortified cereals, and egg yolks are common dietary contributors. Still, readers often discover that food alone may not reliably correct low vitamin D status.
Sunlight can help the body synthesize vitamin D, but sun exposure during pregnancy must be approached thoughtfully. Skin protection, heat tolerance, and risk reduction for hyperpigmentation are practical concerns. Many prenatal guidance discussions encourage a “measured” approach: enough exposure to support vitamin D pathways, without compromising skin safety.
Supplementation: Choosing Dose, Timing, and Form Responsibly
Once deficiency is identified—or when risk factors are present—supplementation becomes a structured decision. Vitamin D3 (cholecalciferol) is frequently used because it’s effective at raising 25-hydroxyvitamin D levels. Vitamin D2 (ergocalciferol) may also be used depending on availability and clinical practice.
Timing matters. Some readers expect that starting early in pregnancy might support steadier vitamin D stores, while others are guided by lab results later. This section usually emphasizes individualized care: what’s appropriate depends on baseline levels and whether the goal is maintenance or repletion.
Equally important is safety. Excess vitamin D can lead to hypercalcemia and related complications. The tone here should be cautious and calm: supplementing is not a free-for-all; it’s a precision tool. If readers want the “best practices” feel, this section often lists questions to ask at prenatal visits—target levels, monitoring frequency, and how vitamin D interacts with calcium intake.
What to Expect: Monitoring Blood Pressure Alongside Nutrition
Even if vitamin D is part of the plan, blood pressure management still requires direct measurement. Expect schedules for home monitoring, clinic follow-ups, and trend-based assessment. A narrative that resonates often explains what “trend” means: repeated readings over days or weeks matter more than a single high number.
Some readers are also surprised by lifestyle elements that commonly accompany prenatal BP care: adequate hydration, regular prenatal movement when approved, and minimizing factors that may spike blood pressure. Nutrition threads through the whole fabric, but it’s typically presented as one part of a multi-pronged strategy.
When Vitamin D Isn’t Enough: Recognizing Red Flags and Escalating Care
Gestational hypertension can evolve. Readers need to recognize symptoms that warrant urgent assessment—severe headaches, visual changes, right upper abdominal pain, sudden swelling, shortness of breath, and markedly elevated readings. While vitamin D supports broader health processes, it should never replace medical evaluation.
This section often reassures by clarifying escalation pathways: what to do if readings worsen, when to contact a clinician immediately, and how clinicians decide on additional testing. Short sentences can be lifesaving here: don’t wait, report symptoms, and follow the care team’s instructions.
Types of Content Readers May Find Along the Way
To help readers find their footing, a well-rounded article often includes several content formats. Expect “explainers” that translate medical concepts into everyday language. You may also see “checklists” for questions at prenatal appointments—ideal for turning knowledge into action. Some readers prefer “scenario stories,” where a person’s journey through labs, supplementation, and monitoring is described in realistic steps.
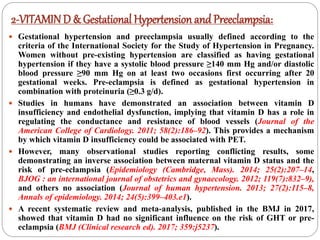
Visual summaries can also help, especially when comparing vitamin D sources, deficiency risk factors, and monitoring intervals. For example, a reader might encounter graphic panels like the kind shown below—useful for reinforcing key ideas at a glance.
Others may encounter downloadable slide-style summaries. These can be especially helpful for readers who like structured repetition—short sections, clear takeaways, and a cohesive pathway through the evidence landscape.
A Thoughtful Bottom Line: Vitamin D as Support, Not a Guarantee
Vitamin D may play a role in pregnancy physiology that intersects with blood pressure regulation—through vascular function, inflammatory balance, and hormonal signaling. Yet the relationship between vitamin D and gestational hypertension is rarely one-dimensional. Readers are likely to find that deficiency correction is a sensible goal, while expectations about blood pressure outcomes should remain appropriately measured.
If you’re considering vitamin D during pregnancy, the most effective approach is usually the most grounded: test when appropriate, supplement thoughtfully under clinical guidance, and continue consistent blood pressure monitoring. Pregnancy care is a collaboration—your body, your lab results, your clinician’s plan, and your daily habits all working together as the story unfolds.




