
When people first encounter drug dosing, two terms often appear like twins separated at birth: the therapeutic dose and the maintenance dose. The common observation is simple—both sound “useful,” both sound “dose-y,” and both appear on dosing schedules. Yet the difference is more than a matter of wording. It is a shift in intent, timing, and pharmacological choreography. The fascination begins when you realize the body is not a passive container. It is an adaptive system, constantly redistributing drug, metabolizing it, and sometimes reshaping the rules of exposure.
Therapeutic Dose: The Intended Clinical Spark
A therapeutic dose is the dose administered to produce a desired clinical effect. It is the dose chosen to reach a therapeutic goal—relief of symptoms, suppression of a disease process, or achievement of a measurable pharmacodynamic outcome.
In everyday practice, the therapeutic dose is often the starting point for thinking: “Will this amount actually work?” But that question hides a deeper complexity. The therapeutic dose must land the drug within an effective range—commonly framed as a target concentration window in pharmacokinetics. If the dose is too low, effect fails to materialize. If too high, toxicity may become the loudest voice in the room.
Therapeutic dosing also tends to be shaped by the medicine’s onset requirements. Some conditions demand rapid action, while others tolerate gradual correction. Consequently, the therapeutic dose may involve loading strategies in certain drug classes, because waiting for equilibrium can delay clinical benefit.
Maintenance Dose: The Art of Staying Put (Without Staying Too Much)
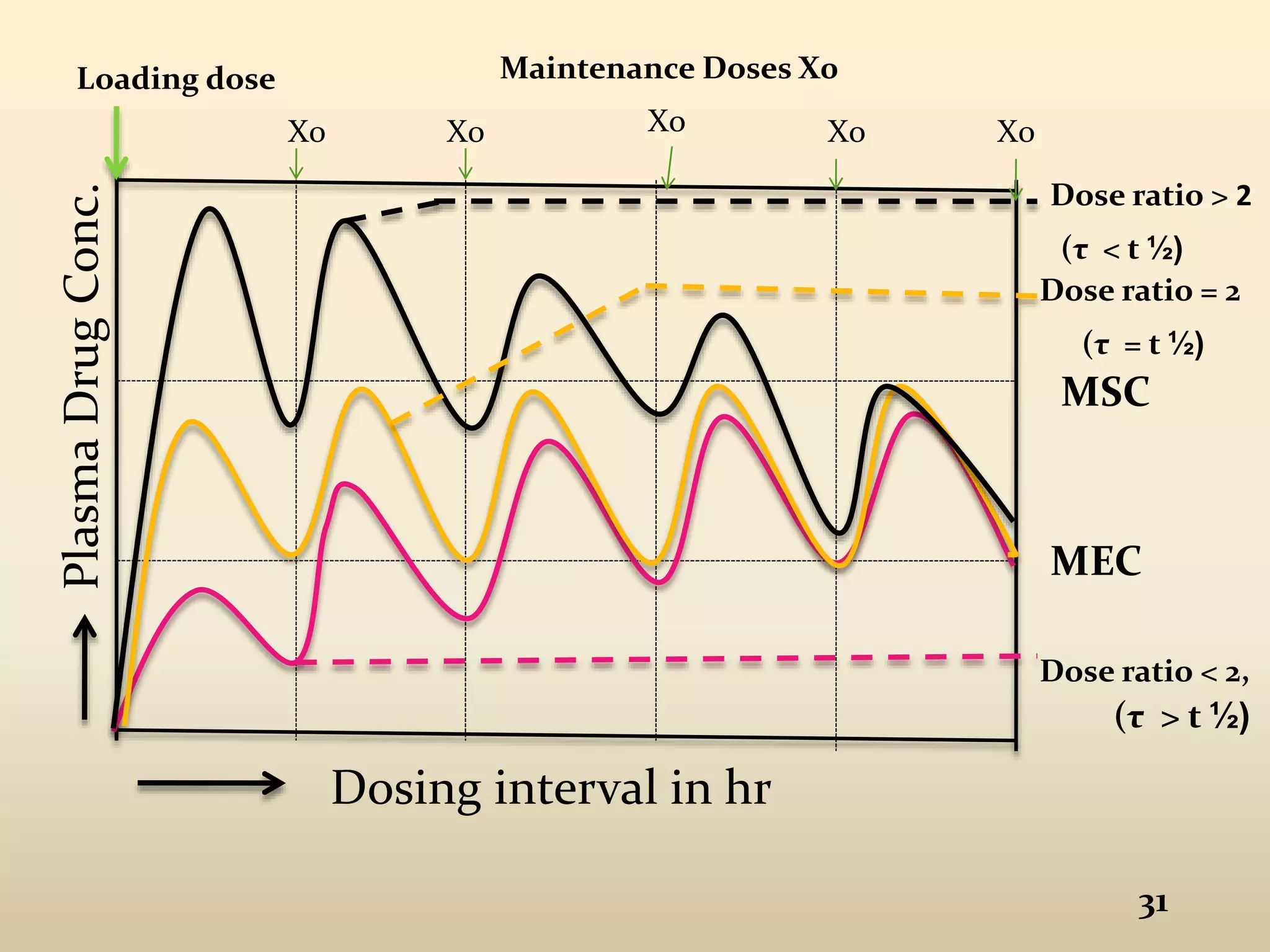
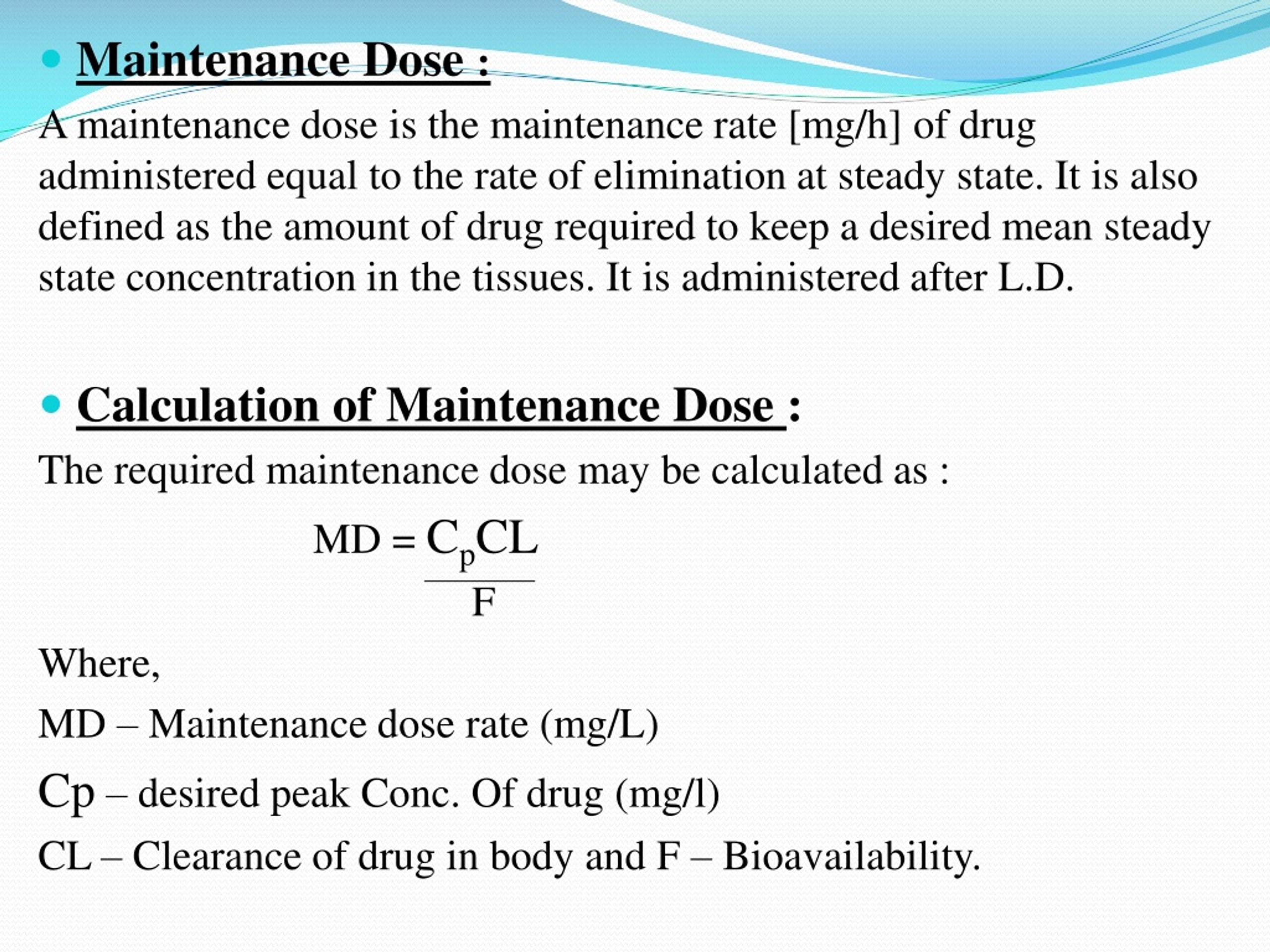
A maintenance dose is the dose given to sustain a therapeutic effect over time. The purpose is less about initiating benefit and more about preventing decline—preventing the drug concentration from slipping below the effective threshold.
If the therapeutic dose is the opening chord, the maintenance dose is the recurring rhythm that keeps the song from drifting into silence. After the body absorbs and distributes the drug, elimination—through metabolism and excretion—begins to steadily lower drug levels. Maintenance dosing is designed to counter that downward trend.
Importantly, maintenance dosing depends on the drug’s half-life and clearance dynamics. Even when a therapeutic dose successfully reaches the target range, the pharmacokinetic curve does not flatten by virtue of optimism. The concentration will fall unless replenished at an appropriate interval and amount.
This is where a common misconception emerges: people sometimes assume maintenance dose is merely “a smaller therapeutic dose.” Not always. Maintenance dose is defined by timing plus sustained exposure, not by size alone. A drug with a long half-life may require infrequent dosing; another with rapid clearance may require more frequent administration—even if each dose appears modest.
The Fundamental Difference: Goal and Phase of Treatment
The difference can be summarized as a shift in treatment phase.
Therapeutic dose focuses on achieving the initial clinical effect, often early in therapy. It answers, “Can we turn the effect on?”
Maintenance dose focuses on preserving the effect and preventing both relapse and subtherapeutic drift. It answers, “Can we keep the effect on without overshooting?”
Both doses are therapeutic in their own way, but they occupy different roles in the arc of pharmacological time. Therapeutic dosing is about reaching; maintenance dosing is about holding. This temporal distinction is not pedantic—it reflects how drug concentrations rise, peak, and decline in real biological conditions.
Pharmacokinetics Behind the Curtain: Absorption, Distribution, Elimination
Underneath the vocabulary is a sequence of kinetic events. After administration, a drug undergoes:
Absorption (entering systemic circulation), distribution (spreading into tissues), and elimination (metabolism and excretion). The therapeutic dose must overcome early variability—how quickly the drug arrives and how effectively it permeates relevant tissues.
Maintenance dosing, by contrast, is largely about the equilibrium between elimination and dosing frequency. When dose intervals are misaligned with clearance, the concentration curve begins to wobble: troughs sink below efficacy, peaks flirt with toxicity, and the patient becomes an unwitting participant in a pharmacokinetic experiment.
The fascination deepens here. A stable regimen is essentially a negotiated peace between the body’s removal machinery and the dosing cadence. When clinicians adjust a maintenance dose, they are not guessing blindly. They are recalibrating a dynamic system.
Therapeutic Index and the Tightrope of Safety
Both therapeutic and maintenance dosing must respect the therapeutic index—the margin between effective and harmful concentrations. Yet the maintenance phase introduces a subtle risk: long-term therapy can accumulate consequences even when each individual dose is “reasonable.”
With maintenance dosing, the goal is steady-state exposure. That steady state is not an instant gift; it typically develops after multiple dosing intervals. During the approach to steady state, concentrations may be transitioning, and the regimen must be designed so that the patient does not suffer through peaks too high or troughs too low.
This is why clinicians may use dose adjustments, therapeutic drug monitoring, or careful titration. The regimen becomes individualized—shaped by metabolism rates, organ function, drug interactions, adherence patterns, and sometimes genetic variability.
Why Maintenance Dose Can Be “Required” Even When Therapeutic Dose Worked
A common observation is: “If the therapeutic dose achieved the effect, why not stop?” The deeper reason is elimination. The body continues to metabolize and excrete the drug, so the concentration cannot remain in the therapeutic range without replenishment.
Think of it as a lighthouse beam. The therapeutic dose is like turning on the light to signal safely. But the mechanism of survival requires ongoing operation. Maintenance dosing ensures the beam returns each cycle before darkness wins.
Stopping after the therapeutic dose may yield temporary improvement, then deterioration. Maintenance dosing prevents the oscillation that can occur when drug levels fall below the effective threshold.
Individualization: The “Same Name” Dose, Different Physiological Reality
Therapeutic dose and maintenance dose are not universal constants. Two patients can receive identical milligram values yet experience different exposure because of differences in clearance, body composition, age, hepatic or renal function, and concomitant medications.
Uncommon but useful terminology helps capture this: clearance and bioavailability create a pharmacological fingerprint for each patient. Maintenance dosing is essentially an attempt to match that fingerprint with a target exposure profile.
In practice, dose schedules can be adjusted based on measured drug concentrations, clinical response, and tolerability. This transforms dosing from a rote prescription into a calibrated intervention.
Putting It Together: A Cohesive View of the Dosing Story
Therapeutic dose is the dose that aims to initiate or achieve a clinical effect; maintenance dose is the dose that preserves that effect through time. The difference is not merely quantitative—it is temporal and mechanistic.
Once you see dosing as a dynamic relationship between administration and elimination, the terminology stops feeling arbitrary. It becomes a map of intent: reach the therapeutic range, then remain within it.
And that is the deeper fascination. Dosing is not only about chemistry. It is about timing, feedback, and the patient’s evolving physiology. Every regimen is a small, deliberate negotiation between medicine and biology—one that continues long after the first dose does its work.




