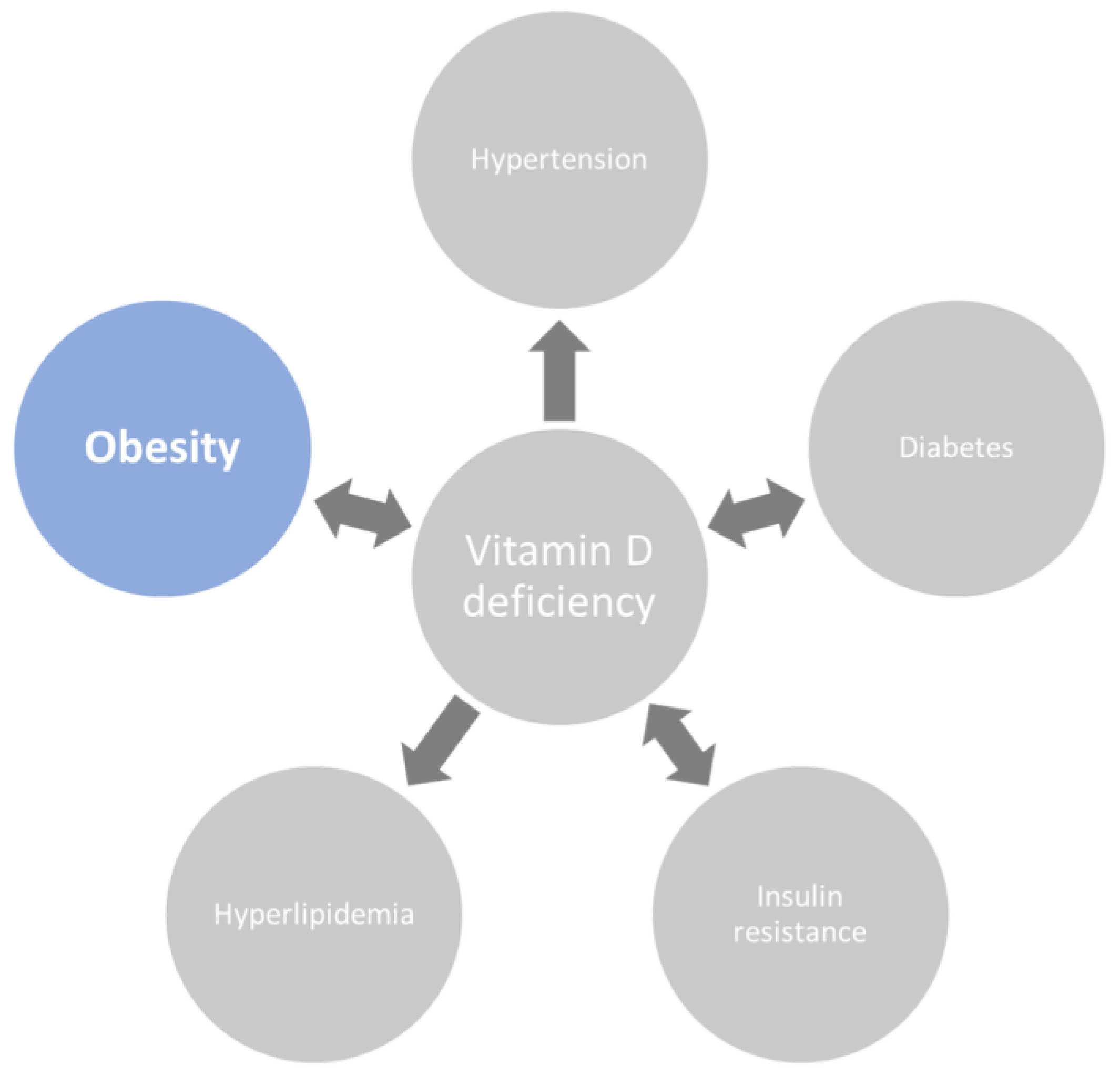
Obesity is often treated as a problem of excess calories alone, yet the body rarely obeys such simple bookkeeping. One quietly persistent consequence is low circulating vitamin D. It can feel paradoxical—vitamin D is forged in the skin through sunlight, and diet can supply a fraction—but obesity can still drag levels downward. A major reason involves sequestration in fat: vitamin D gets stored, buffered, and effectively “held hostage” inside adipose tissue, leaving less available in the bloodstream when the body needs it most.
Adipose Tissue as a Vitamin D “Sponge”
To understand sequestration, imagine adipose tissue as a high-capacity reservoir with many small compartments. Vitamin D is fat-soluble. That single trait changes the entire distribution story. When vitamin D enters the circulation, it does not behave like a water-soluble nutrient that freely travels and quickly equilibrates. Instead, it prefers lipid-rich environments. In obesity, there is simply more lipid territory to absorb and store vitamin D.
Over time, the storage effect becomes conspicuous: vitamin D that might otherwise remain bioavailable is sequestered inside fat cells. Short sentences matter here because the mechanism is direct: more adipose mass means more storage volume. Less adipose “spillover” means less vitamin D circulating for endocrine use.
Fat Compartmentalization and Delayed Release
Sequestration is not only about holding vitamin D—it’s also about timing. Fat cells can act like slow-turning vaults. Even when vitamin D is present in adipose tissue, its release may be sluggish. This creates a temporal mismatch: sunlight exposure or supplementation may increase total stores, yet serum levels can remain depressed because the circulation receives only a fraction of what has been captured.
Think of it as a buffering phenomenon. The body can accumulate vitamin D stores while simultaneously experiencing functional insufficiency in the bloodstream. The result is a pattern many clinicians recognize: total body vitamin D may not reflect the level that peripheral tissues can access easily.
Obesity also tends to create chronic metabolic turbulence—low-grade inflammation, oxidative stress, and altered endocrine signaling. These conditions may further influence how vitamin D is handled, retained, and mobilized, even if sequestration is the primary anchor of the explanation.
Visceral Fat: A Particularly Potent Reservoir
Not all fat is equal. Visceral adiposity—the fat stored around organs—has a distinct metabolic character. It is more hormonally active and more tightly linked to insulin resistance and inflammatory signaling. Vitamin D sequestration can be more pronounced when adiposity is concentrated in these compartments.
In practical terms, two people might have the same body mass index, but different distributions of fat. The person with a higher proportion of visceral fat may experience a greater decline in serum vitamin D availability. The “where” matters, not just the “how much.”

Lower Bioavailability: When Total Stores Don’t Translate to Function
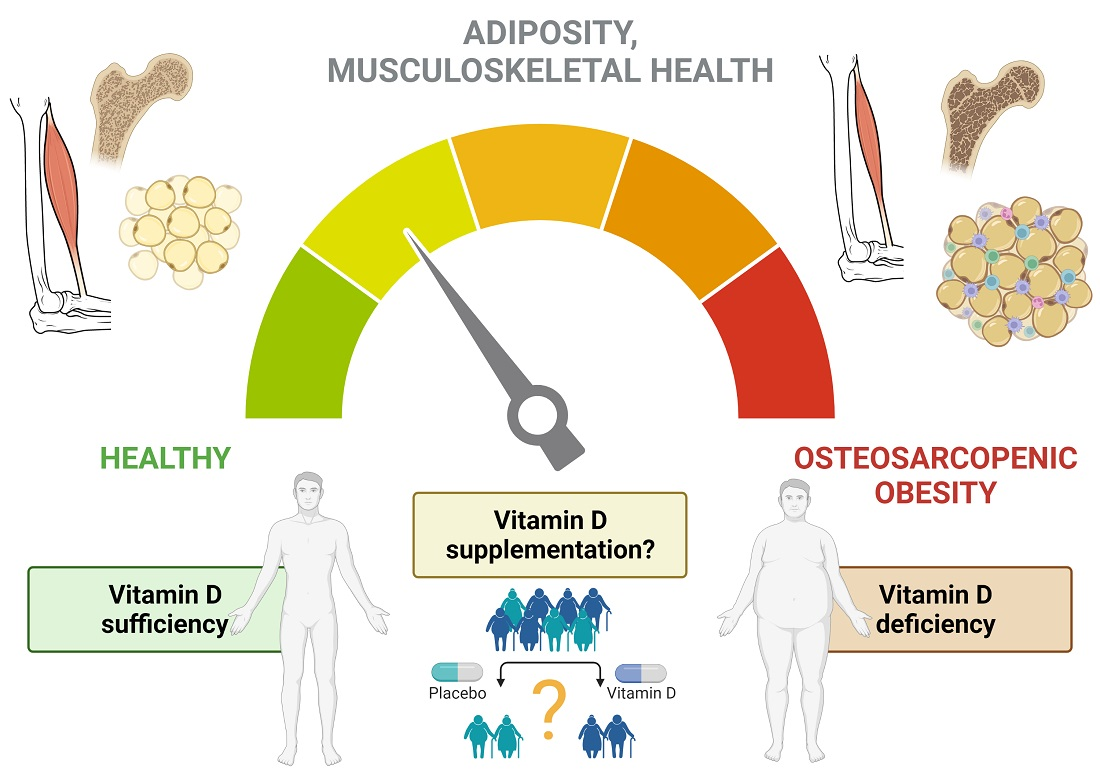
Serum vitamin D is often measured as 25-hydroxyvitamin D, a marker used as a proxy for vitamin D availability. Sequestration can distort the relationship between measured stores and real-time functional needs. Even if vitamin D is “somewhere” in the body—cached in fat—it may not be delivered efficiently to tissues that depend on it for regulation of immune function, musculoskeletal health, and broader metabolic signaling.
This is where biochemical nuance becomes clinically meaningful. Vitamin D’s downstream roles involve conversion and receptor-mediated actions. If circulating levels remain low, the cascade toward active metabolites may be under-supplied. The sentence to remember: low serum availability can persist even when the body has abundant lipid-rich storage capacity.
In other words, obesity can convert vitamin D from a circulating hormone-like nutrient into a compartmentalized substrate.
Inflammation, Adipokines, and the Metabolic Feedback Loop
Vitamin D interacts with immune regulation and inflammatory pathways. Obesity, meanwhile, is characterized by a persistent low-grade inflammatory milieu and altered adipokine signaling. This bidirectional interplay can deepen the cycle: inflammation may influence vitamin D metabolism and receptor activity, while insufficient vitamin D can fail to dampen inflammatory signals.
Sequestration helps explain the initial drop, but inflammation can extend the problem. Think of a feedback loop with two gears. One gear is physical—lipid sequestration. The other is biochemical—inflammatory and endocrine signaling. When both engage, deficiency can become more entrenched.
Short, crisp patterns often emerge. People with higher adiposity frequently show lower vitamin D. Over time, their biochemical environment makes correction more complex than simply taking a supplement.
Why Sunlight Exposure Isn’t Always Enough
Many imagine vitamin D deficiency as a straightforward problem of limited sunlight. But obesity complicates this logic. Skin exposure may not translate into adequate serum rises because vitamin D formed or ingested must still distribute and remain bioavailable. Sequestration works like a sink that continues to absorb what arrives.
Even when sunlight exposure improves, the body may continue to partition newly available vitamin D into fat stores rather than letting serum concentrations climb as expected. This creates a “ceiling effect” in practical outcomes: supplementation and modest sun exposure may raise total reserves, but serum improvement can be muted.
In narrative terms, it feels like trying to fill a reservoir while someone keeps widening the storage cavern around it. The supply does not run out; it just doesn’t accumulate where it’s needed most.
Dietary Patterns, Supplement Absorption, and Practical Expectations
Food provides vitamin D in limited amounts for many people. Some diets include fortified items or fatty fish, while others rarely do. Yet diet alone doesn’t necessarily overcome sequestration. Vitamin D is fat-soluble, and it will still gravitate toward adipose tissue even when obtained via supplements.
Supplementation strategies often face a reality check. Serum levels may respond, but not always proportionally. The dose required to achieve a given serum concentration can be different in individuals with higher body fat. This isn’t a universal rule, but it is a recurring theme in clinical experience.
Readers should expect variable trajectories. Some people correct serum levels relatively well; others experience partial normalization, reflecting how adipose sequestration changes the distribution kinetics.
Type of Content Readers Can Expect: Mechanism, Evidence, and “What To Do Next”
When exploring this topic, readers often benefit from multiple content styles working together. Expect first a mechanistic explanation—how fat-soluble vitamins partition into lipid stores. Next comes interpretive content—why serum levels can remain low even when total vitamin D exists in the body. Finally, practical guidance—how clinicians and patients might set realistic targets and monitor progress.
Mechanistic content is often illustrated with diagrams, lipid partitioning concepts, and compartment models. Interpretive content connects biochemistry to body composition: visceral versus subcutaneous fat, and the difference between storage and availability. Practical content discusses follow-up testing, time horizons, and why response may differ by adiposity.
Short and long sentences should alternate to keep the reader oriented. The short sentences summarize the core idea. The longer ones show how the idea connects to real-world patterns, variability, and metabolic complexity.
The Bigger Picture: Sequestration as One Piece of a Larger Puzzle
Sequestration explains a substantial portion of the link between obesity and low vitamin D, but it isn’t the only factor in the tapestry. Limited sunlight, dietary insufficiency, differences in fat distribution, inflammatory feedback loops, and individual variability in metabolism all contribute. Still, sequestration in fat is a central, intuitive mechanism: more adipose mass offers more storage space for a fat-soluble nutrient.
When you hold that mechanism in mind, the clinical pattern becomes less mysterious. Low serum vitamin D in obesity is not merely an absence of vitamin D—it is a redistribution problem. The vitamin may be present, but it’s locked behind a lipid-rich boundary.
And once you see it that way, the path forward becomes clearer: the goal isn’t only intake, but bioavailability—ensuring that enough vitamin D remains in the circulation to perform its roles throughout the body.



