What if a simple nutrient—quiet, sun-powered, and often overlooked—could nudge depression toward remission? Now here’s the playful twist: the same vitamin D that feels like “good vibes” might be the very thing your mood needs most… or at least, that’s what the evidence hints. Yet the challenge lands early—because “ideal” is an unruly word in real life. Different studies measure vitamin D differently, cut their thresholds differently, and watch mood change at different rhythms. So what level is truly “ideal” for depression remission?
First, a quick detour: What counts as “vitamin D level”?
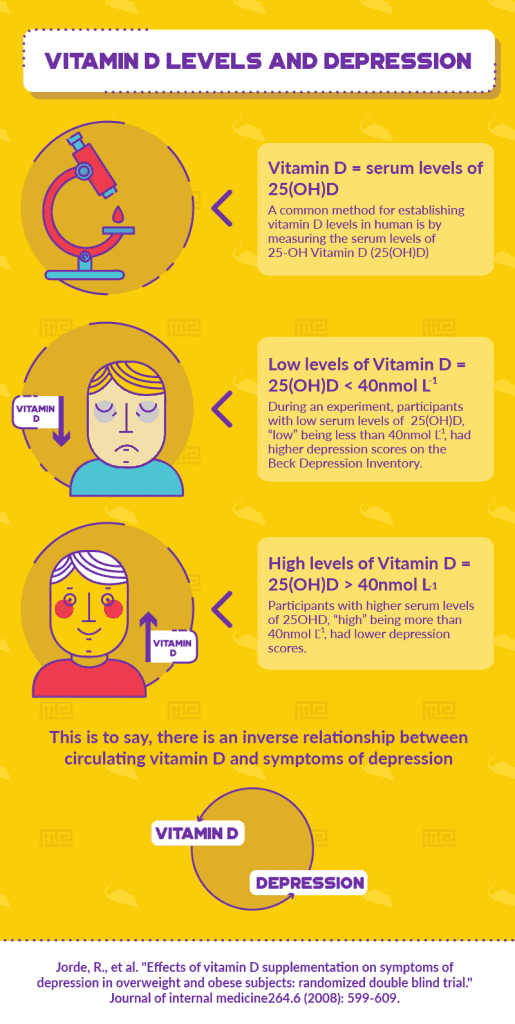
Vitamin D is commonly assessed through 25-hydroxyvitamin D (25(OH)D). This marker is the circulation’s best snapshot of vitamin D availability. Blood tests typically report it in ng/mL or nmol/L. A lab might report “low,” “insufficient,” and “sufficient” using its own grading ladder—so two people can both be “not ideal,” but by different yardsticks.
Why does this matter? Because depression remission isn’t a binary switch. It’s a moving target. When researchers compare vitamin D levels with depression outcomes, they’re often sifting through a complex cloud of confounders: baseline severity, sun exposure, diet, medication type, physical activity, and even seasonality.
So what “ideal” level is commonly suggested?
In broad clinical discussions, many guidelines treat roughly 20 ng/mL as a threshold for adequacy, while some argue that 30 ng/mL (and sometimes higher) better reflects optimal physiological function. For depression specifically, evidence tends to cluster around an idea: higher vitamin D status—especially when moving out of deficiency—may correlate with improved depressive symptoms and, in some groups, with remission.
However, the “ideal” value is less a single number and more a probabilistic zone. Some studies show benefit as people rise from low to moderate levels. Others suggest diminishing returns once levels are already adequate. A few report associations primarily in those who were deficient or severely low to begin with. In other words, the “ideal” may be conditional: it may depend on where you start.
Think of it like tuning a radio. If you’re listening to static, any adjustment can sound like progress. If you’re already tuned, small turns may not dramatically improve the signal.
Depression remission: how vitamin D might be involved
Vitamin D isn’t merely a bone-supporting actor. It functions more like a hormonal regulator—quietly influencing neurobiology, immune signaling, and cellular resilience. Several plausible pathways have been proposed:
Neurotransmitter modulation: Vitamin D may influence systems tied to serotonin and other mood-related signaling pathways.
Inflammation tempering: Depression has been linked with inflammatory activity in many patients. Vitamin D can modulate immune responses, potentially reducing inflammatory noise.
Neuroprotection: Some research suggests vitamin D supports brain health through mechanisms related to neuroplasticity and oxidative stress.
None of these pathways prove causation on their own. But together, they make a coherent narrative: vitamin D could create a biochemical environment where mood improvement is more likely—especially during treatment.
What the evidence tends to show: remission is not just correlation
When studies examine vitamin D alongside depression outcomes, patterns often look like this: people with lower vitamin D levels are more likely to have persistent depressive symptoms, while those with higher levels may have better odds of improvement or remission. Yet the evidence is not uniform. Some trials suggest supplementation can help, others find minimal or inconsistent benefit.
Why might this happen? Several factors complicate the picture:
Baseline status: Supplements are more likely to show benefit when a participant is actually deficient.
Dose and regimen: A one-size dosing plan is rarely “ideal.” Frequency, total dose, and adherence vary.
Time horizon: Mood change takes time. Vitamin D repletion may occur over weeks to months, but remission depends on the interplay with therapy and medication.
Measurement variability: Sun exposure, skin pigmentation, latitude, clothing, and seasons can shift levels quickly.
So when researchers propose an “ideal” level, they’re often describing where benefit seems to cluster—rather than guaranteeing an outcome for every individual.

Could too little vitamin D be the “hidden antagonist”?
Here’s the potential challenge—one that feels almost mischievous. Depression treatment often focuses on brain chemistry, behavior, and coping strategies. But vitamin D is frequently treated as a side quest. If someone is deficient, their recovery might be fighting an uphill battle at the biochemical level.
Imagine two people starting antidepressant therapy. One has adequate vitamin D and the internal “regulatory channels” are already functioning with less friction. The other begins with deficiency, and their system may be less equipped for the biological processes linked to mood stabilization. The second person might still improve, but perhaps with a slower or less complete arc—unless vitamin D status is addressed.
This doesn’t mean vitamin D replaces standard depression care. It means it may act as a supportive variable—one that can strengthen the odds when deficiency is present.
What about supplementation—can you “reach ideal” safely?
Supplementation can raise vitamin D levels, but safe practice matters. Excess vitamin D can lead to hypercalcemia and related complications. That’s why the most prudent approach is individualized: test first, supplement with appropriate dosing, then recheck levels.
Clinicians often aim to move people toward adequacy—frequently in the 20–30 ng/mL range, with some aiming higher depending on patient context. But “aiming higher” should not become a reflex. Depression remission is the target; safety is the boundary.
Consider this: if you chase an arbitrary number without monitoring, you might improve the lab value while ignoring the rest of the clinical picture. Mood is not a vitamin meter; it’s a multi-system phenomenon.
How to think about “ideal” for you specifically
“Ideal” might depend on your starting point, your season, your treatment plan, and your overall health. A reasonable mental model is to treat vitamin D as one component in a larger remission strategy—like checking the thermostat while also tuning airflow and insulation. Helpful, but never the whole house.
Ask practical questions:
What is your measured 25(OH)D level?
Is it deficient, insufficient, or already adequate?
How stable is your sun exposure across the year?
Are you taking meds or supplements that affect vitamin D or calcium?
What other factors are influencing depression remission?
By framing “ideal” as a personalized target grounded in testing, you trade vague hope for measured progress.
The bottom line: a number, a zone, and a careful next step
The evidence most often points to a hopeful conclusion: maintaining an adequate—and sometimes closer to the upper end of sufficiency—vitamin D status may be associated with better depression outcomes, including remission. Yet the “ideal” is best understood as a range and a context-dependent threshold, especially because people with deficiency appear more likely to benefit.
So the playful question returns, slightly revised: what if remission needs more than willpower and prescriptions? What if it also needs the biochemical foundation that vitamin D may help provide?
If you’re considering this path, the most powerful move is simple: get a 25(OH)D test, discuss results with a clinician, correct deficiency responsibly, and continue evidence-based depression care. Vitamin D might not be the hero of the story—but in the right chapter, it can be the supportive co-star that helps the plot finally soften toward remission.



