Vitamin D sits at an unusual crossroads in human biology: part hormone, part immune “modulator,” and—when levels run low—part conspirator in the inflammatory story many people with autoimmune conditions come to know all too well. For individuals living with multiple sclerosis (MS), lupus, or rheumatoid arthritis (RA), the question often isn’t whether vitamin D matters, but what “dose” actually means, how it is tailored, and how it can be integrated into an overall, evidence-informed care plan. Dosing is never one-size-fits-all; it is more like a carefully tuned instrument, calibrated to bloodwork, body composition, sun exposure patterns, medications, and the pace of disease activity.
Why Vitamin D Becomes Relevant in Autoimmunity
Autoimmune disease involves the immune system misidentifying the body’s own tissues as threats. Vitamin D helps shift immune responses toward a more regulated profile. It influences innate and adaptive immune signaling, including the behavior of antigen-presenting cells and the balance between pro-inflammatory and anti-inflammatory pathways. In practical terms, sufficient vitamin D may support a calmer immune environment—though it does not “cure” autoimmune disease and it does not replace disease-modifying therapy.
When vitamin D is insufficient, the immune system can become more reactive, and inflammatory cascades may gain momentum. This is where dosage enters the narrative: dosing aims to correct a deficiency, maintain an adequate level, and reduce the probability that chronic low vitamin D quietly amplifies immune dysregulation.
The First Step: Understanding Your Baseline (25(OH)D)
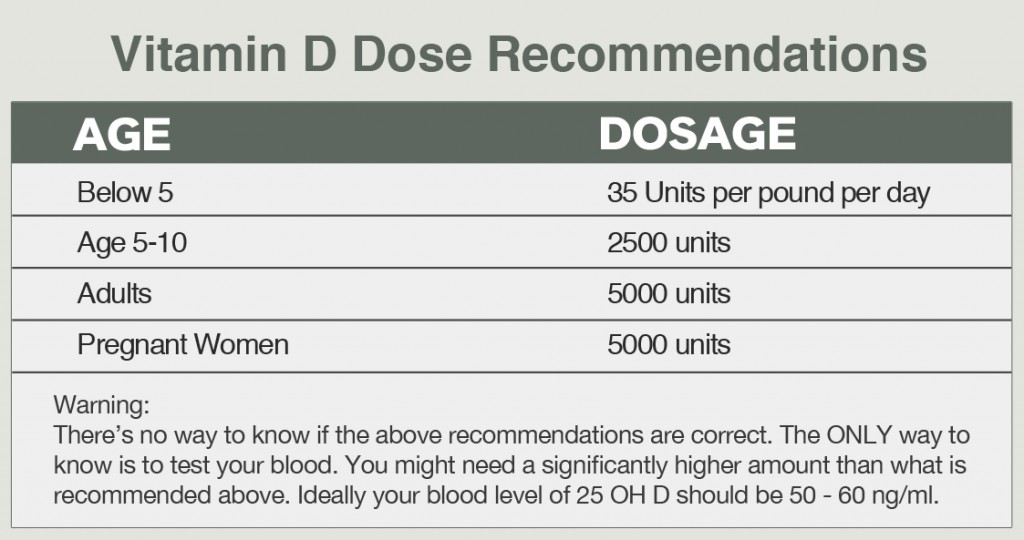
The dosing conversation begins with the metabolite most clinicians measure: 25-hydroxyvitamin D, written as 25(OH)D. This is the bloodstream indicator that reflects total vitamin D from sun exposure, diet, and supplements. Without that baseline, dosing can be guesswork—sometimes under-correcting, sometimes overreaching.
Typical lab reporting units may vary by country. The value guides decisions such as whether to use a loading strategy (brief, higher dosing to rebuild stores) or a maintenance strategy (steadier, lower dosing to sustain levels). A useful narrative checkpoint is to ask: Are we addressing a deficiency, maintaining sufficiency, or trying to nudge a borderline level upward?
General Dosing Frameworks (What “Dose” Commonly Means)
Most vitamin D dosing strategies fall into two phases. The first is replenishment—often used when 25(OH)D is low. The second is maintenance—used after levels stabilize. Replenishment may require larger daily doses or occasional higher-dose regimens, depending on clinician preference, patient tolerance, and comorbidities.
Commonly used daily supplement doses often range from modest amounts to higher daily totals. For example, some people remain in the 800–2,000 IU/day neighborhood for maintenance, while others may be prescribed higher amounts if their levels are significantly deficient. The key detail is not the number itself—it is the measured response: repeat lab testing after a sensible interval helps confirm that dosing is landing where it should.
Short sentences matter here because dosing is iterative. You raise. You retest. You adjust. Over time, the plan becomes individualized rather than generic.
Target Levels: What Many Clinicians Aim For
There is no universal target that every guideline agrees on in every clinical scenario, but many clinicians aim to keep 25(OH)D within a range associated with sufficiency for bone and immune function. Levels that are too low may correlate with worse inflammatory outcomes, while extremely high levels can increase risk—particularly hypercalcemia.
Autoimmune disease adds complexity. Some patients may be more prone to deficiency due to reduced sun exposure, higher body weight (which can dilute vitamin D stores), or medication effects that indirectly influence metabolism. That means targets are often treated as practical goals rather than abstract numbers.
In MS, lupus, and RA, the vitamin D plan should also remain compatible with concurrent therapies such as corticosteroids, immunosuppressants, and disease-modifying agents. A cohesive regimen protects both inflammatory control and metabolic safety.
MS (Multiple Sclerosis): Dosing Considerations and Timing
In MS, vitamin D has been studied as a potential immune-regulatory factor. While it is not a stand-alone treatment, adequate vitamin D status is frequently viewed as a supportive lever. Dosing often depends on how low the starting level is and whether the patient has limited sun exposure or frequent disease flares.
Some patients wonder whether dosing should be “more aggressive” during flare periods. In reality, most approaches still emphasize achieving and maintaining sufficiency consistently, because immune regulation is unlikely to behave like an on-off switch. If a flare occurs, the priority is managing MS activity through established therapy; vitamin D may support the background immune milieu but should not become a substitute.
Long sentences can be tempting here, but the practical takeaway is simple: dose based on labs, adjust based on response, and reassess at appropriate intervals—often after several months of supplementation.
Lupus: Balancing Deficiency Correction With Whole-Body Care
Lupus can include photosensitivity, and photosensitivity often translates into less sun exposure. That reduces natural vitamin D synthesis, increasing the likelihood of deficiency. Dosing strategies in lupus often focus on correcting insufficiency while supporting overall wellness—especially because lupus management frequently involves multiple moving parts: inflammation control, kidney monitoring, and cardiovascular risk reduction.
Kidney involvement can complicate vitamin D metabolism. If kidney function is impaired, vitamin D handling may differ, and calcium balance becomes more delicate. Therefore, dosing should be guided not only by 25(OH)D but also by clinician oversight of labs that reflect mineral metabolism.
In lupus narratives, vitamin D supplementation is often woven into a broader regimen: hydration, careful medication adherence, and vigilant lab monitoring. The immune system does not live in a vacuum, and neither does supplementation.
RA (Rheumatoid Arthritis): Consistency and Measurement
RA is characterized by chronic inflammation and immune dysregulation, often requiring long-term medication. Vitamin D can be considered a supportive cofactor—particularly because low vitamin D levels are common and because RA patients may have lifestyle factors that limit sun exposure.
Dose selection in RA tends to emphasize consistency. Steady supplementation is usually preferred over sporadic high dosing, unless a clinician is using a deliberate replenishment approach. The goal is to maintain a stable 25(OH)D level rather than chase fluctuations.
Short bursts of dosing can be useful for repletion, but long-term success typically depends on maintenance and follow-up. A clinician might schedule repeat testing after a reasonable adjustment window, then fine-tune dosage.
Forms of Vitamin D: D2 vs D3 and Practical Absorption Tips
Vitamin D comes primarily as D2 (ergocalciferol) and D3 (cholecalciferol). Many people respond better with D3 in real-world settings, but individual responses still vary. What matters most is supplement quality, dose accuracy, and consistent intake.
Absorption can improve when vitamin D is taken with meals that contain fat. Because vitamin D is fat-soluble, diet composition can influence the degree to which the body absorbs and retains it. Consistency is not boring—it is biochemical.
Some patients also choose liquid forms for dose flexibility, while others prefer capsules or tablets. The “best” form is the one that supports adherence and reliable dosing.
Safety: Upper Limits, Calcium Monitoring, and Red Flags
Vitamin D is not harmless at excessive levels. Too much can raise calcium, leading to symptoms such as nausea, constipation, excessive thirst, frequent urination, fatigue, confusion, or kidney-related discomfort. These signs are not diagnostic by themselves, but they are red flags that warrant prompt medical attention.
Safety is especially important for autoimmune patients who may have comorbidities or who take medications that affect mineral balance. Clinicians may monitor calcium, kidney function, and vitamin D levels, especially when higher doses are used.
Long-term, the safety story is a stewardship story: dose with intention, recheck levels, and avoid “set it and forget it” behavior.
Medication Interactions and Overlapping Lab Concerns
Autoimmune therapy often includes glucocorticoids, immunosuppressants, and other agents that can indirectly influence bone health and metabolism. Corticosteroids, for instance, are well known for impacting bone density—so vitamin D supplementation can become part of a bone-protective strategy. Still, vitamin D must be coordinated with calcium intake and, when appropriate, other bone-supporting interventions.
Interactions can also occur through changes in how vitamin D is processed in the body. That is why lab-guided dosing is so valuable: it accounts for individual metabolism rather than relying purely on a generic prescription.
If your care plan includes multiple supplements—calcium, magnesium, vitamin K, or multivitamins—ensure there is no unintended stacking that drives totals too high.
What Content Readers Can Expect From a Smart Dosing Plan
A complete plan typically contains three content layers. First, it offers the “how” (what dosage strategy is being used—repletion or maintenance). Second, it offers the “proof” (which labs are being monitored and when). Third, it offers the “safety narrative” (upper thresholds, symptom awareness, and risk reduction).
In addition to dosing details, many clinicians also integrate lifestyle guidance: safe sun exposure when feasible, dietary sources of vitamin D, and attention to body-weight considerations. Readers should expect a dosing approach that respects individuality rather than delivering a single universal number.
Finally, a high-quality dosing strategy includes a feedback loop. Vitamin D is not static; disease activity, medications, and seasonal sun exposure can change over time. Reassessing levels and adjusting dosage helps keep the plan aligned with the body’s current reality.
Putting It All Together: A Cohesive Next Step
For MS, lupus, and RA, vitamin D dosage is best understood as a managed, measurable intervention. Start with a 25(OH)D blood test, choose a replenishment or maintenance approach based on that result, and adjust after follow-up testing. Prioritize safety by monitoring calcium and relevant labs when higher doses are used or when comorbidities exist.
Consistency is the quiet engine behind most success stories. Dose thoughtfully, retest reliably, and coordinate with the overall autoimmune treatment plan. In that context, vitamin D becomes more than a supplement—it becomes a structured, evidence-guided ally within a comprehensive care narrative.




