
After 40, the body begins to negotiate in smaller, quieter ways. The dance between vitamin D and parathyroid hormone (PTH) is one of those subtle negotiations—yet it can decide whether bones feel resilient or increasingly fragile. This isn’t just chemistry on paper. It’s the hidden steering wheel that influences calcium availability, bone remodeling tempo, and the long-term texture of skeletal health.
The Quiet Metronome: What Vitamin D Actually Does
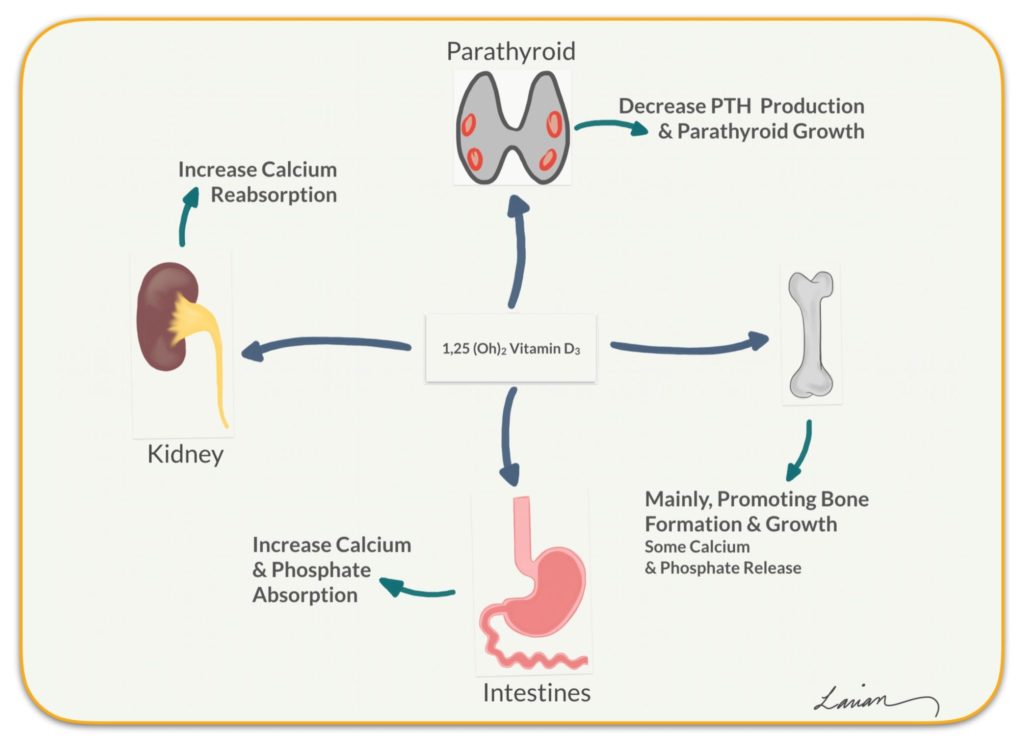
Vitamin D is often treated like a simple “supplement” word. But inside the body, it behaves more like a regulatory messenger. Its most essential role is to help the intestine absorb calcium. Without sufficient vitamin D, calcium absorption can become inefficient, even if calcium intake is reasonable.
Now consider what happens next. When calcium absorption underperforms, blood calcium levels may dip toward the lower edge of normal. The body rarely tolerates even small imbalances for long. It prefers stability, because stability is survival.
So vitamin D is not merely “about bones.” It is about the boundary conditions that keep calcium steady enough for nerve conduction, muscle contraction, and—crucially—bone maintenance.
And here is the intriguing twist: the further you move from optimal vitamin D status, the more your body may rely on backup systems, some of which can be expensive to bone tissue over time.
Parathyroid Hormone: The Emergency Planner with a Double-Edged Edge
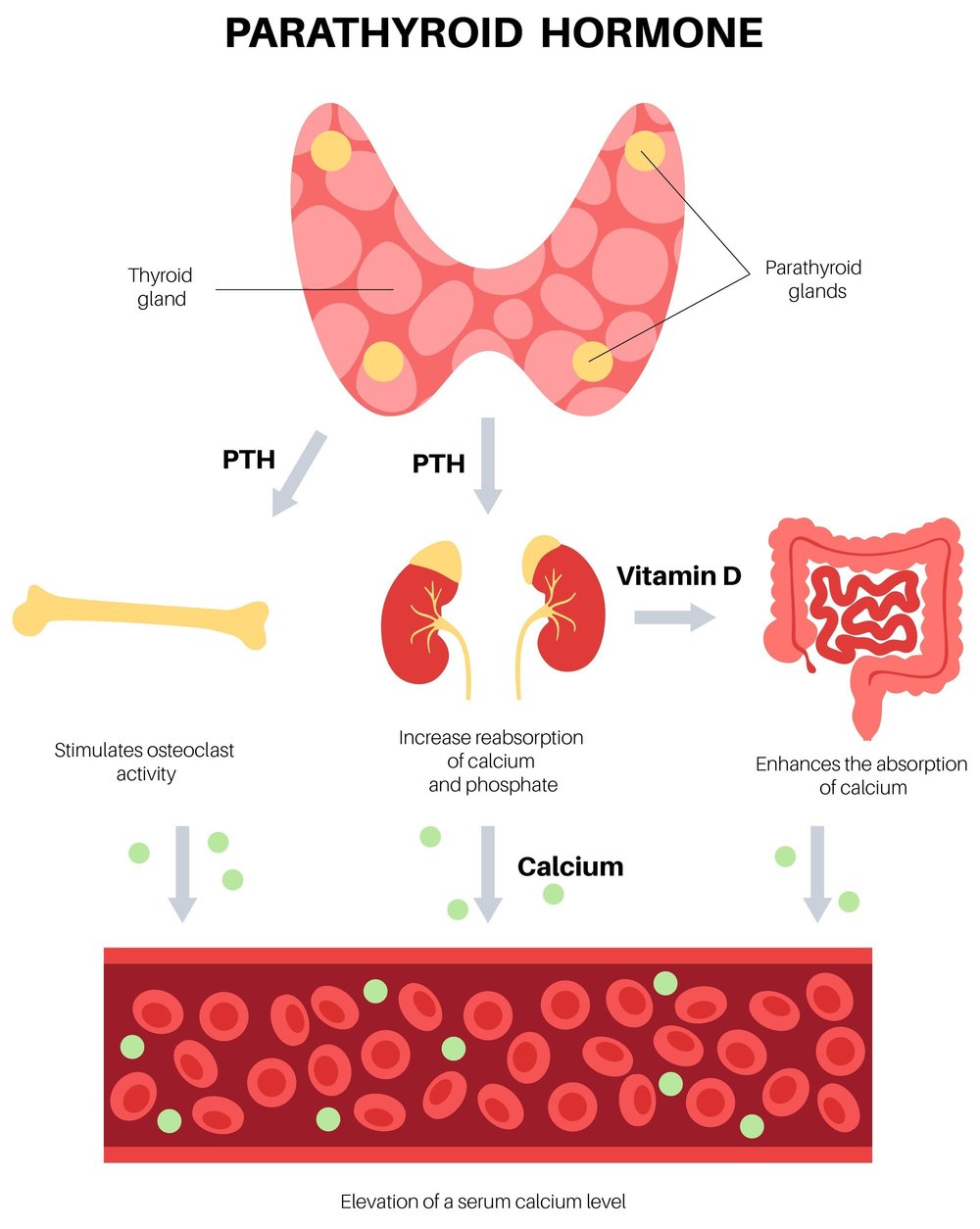
PTH is released by the parathyroid glands when the body senses that calcium levels are too low. Think of it as an emergency planner. It can rapidly mobilize calcium—so the blood stays stable.
But emergencies tend to create tradeoffs. Chronic or repeatedly elevated PTH may increase bone resorption, meaning bone is broken down to liberate calcium. This doesn’t happen overnight. Instead, it often accumulates like fine dust settling into the grain of time.
In younger years, the hormonal feedback loop can be more forgiving. After 40, however, several factors can make calcium management less efficient—less robust vitamin D synthesis in the skin, changing kidney handling of minerals, and a general shift in how the body responds to signals.
The result can be a scenario where PTH stays “just a bit high,” not enough to cause dramatic symptoms, but enough to nudge the bone remodeling balance in a less favorable direction.
The Bone Balance Equation After 40: Remodeling Isn’t Optional
Bones are not static scaffolding. They are living organs with remodeling cycles—building and breaking happen continuously. Osteoblasts construct, while osteoclasts dismantle. Healthy balance yields strong architecture. Imbalanced signals can tilt the scale toward breakdown.
Vitamin D and PTH sit at the center of this tilt. Vitamin D supports calcium absorption and also influences bone cells directly, modulating how they respond to mineral availability. PTH influences bone turnover. When vitamin D is sufficient, PTH can stay in a healthier range because the body has less need to “pull” calcium from bone.
After 40, even small deviations can matter. Bone remodeling rates may change, and the “quality control” of mineralization can become less precise. The skeleton may still repair itself—but the repair may be slower, and the margins for error narrower.
This is where a shift in perspective becomes powerful: you’re not only preventing deficiency. You’re optimizing the hormonal climate that governs bone’s internal decisions.
Why Vitamin D Deficiency Can Be Deceptively Silent
Many people associate vitamin D deficiency with obvious signs—yet deficiency can creep in without dramatic warnings. Fatigue, vague aches, or a general sense of “sluggishness” may appear, but these symptoms are nonspecific and easy to dismiss.
The body can compensate for a while. It may maintain blood calcium in the normal range while gradually leaning more heavily on PTH. Over time, that compensation can become the pattern.
Consider the psychological trap: “If I feel mostly fine, nothing is wrong.” In mineral metabolism, “mostly fine” can still mean the bone is paying a quiet tax.
Common contributors include limited sun exposure, seasonal changes, darker skin pigmentation (which reduces vitamin D synthesis efficiency), aging skin thickness, and certain dietary patterns. Some medications can also interfere with vitamin D metabolism.
The curiosity-worthy question is this: what if your body is already adjusting—quietly—before symptoms ever appear?
PTH, Vitamin D, and the Calcium Chain Reaction
PTH is not isolated. It interacts with calcium, phosphorus, kidney function, and vitamin D status. One of the most important connections is how vitamin D supports calcium absorption, while PTH encourages bone turnover and helps regulate mineral levels.
When vitamin D is low, calcium absorption decreases. PTH rises to restore calcium. Over time, that increased PTH signaling may foster greater bone resorption. Meanwhile, phosphorus handling can also change, affecting mineralization quality.
This is why clinicians often evaluate multiple labs rather than chasing a single number. A “normal” calcium level can coexist with elevated PTH if vitamin D is insufficient. The skeleton may still be experiencing greater turnover than it should.
The key is to think of bone health as an ecosystem. Calcium is the currency, vitamin D is the exchange rate, and PTH is the policy maker responding to deficits.

Shifting the Mindset: From “Supplements” to “Feedback Loops”
Many people approach vitamin D as a one-time fix: take a pill, move on. But the more useful frame is the feedback loop. Your goals aren’t only to raise a vitamin D number; they are to normalize the hormonal signals that govern bone remodeling.
This means seeing the interplay rather than the isolated component. If vitamin D is inadequate, correcting it may reduce the drive for PTH to compensate. Conversely, if PTH remains persistently elevated despite supplementation, it prompts a deeper look at absorption, kidney function, dietary intake, and other contributors.
It’s a subtle shift—from chasing symptoms to auditing signals. Signals reveal trends. Trends reveal risk before it becomes fracture.
Lab Tests Worth Knowing: What to Ask About
If you want to understand your bone balance, it helps to know which measurements illuminate the pathway. Vitamin D is often assessed via 25-hydroxyvitamin D. PTH can be evaluated to see whether your body is compensating. Calcium may be checked as well, sometimes with additional minerals depending on context.
Because patterns matter, clinicians may interpret results together. For example, vitamin D insufficiency with borderline calcium and higher PTH can suggest that the body is leaning on bone turnover to maintain stability.
Ask for a clear explanation of what your results imply about your endocrine posture—are you maintaining balance through efficient pathways, or through compensatory mechanisms?
Sunlight, Food, and Supplementation: Building a Practical Strategy
Vitamin D can come from sun exposure, diet, and supplements. Sunlight is powerful but variable. Latitude, time of year, cloud cover, skin tone, and sunscreen use all influence how much vitamin D your skin can produce.
Food sources can help, though they may not be sufficient alone for everyone. Fatty fish, fortified dairy or plant alternatives, and certain fortified products contribute. Yet even a thoughtful diet can fall short if baseline status is low.
Supplementation can bridge the gap, but it should be guided by labs and individualized dosing. Overcorrection isn’t beneficial; it can create its own imbalance. The best approach is purposeful: measure, supplement strategically, and recheck to confirm the feedback loop is calming down.
In the background, consistency matters more than intensity. Bones prefer steady, mineral-supportive signals rather than dramatic swings.
When Elevated PTH Isn’t Just About Vitamin D
Here’s where curiosity becomes practical. Elevated PTH can stem from more than vitamin D insufficiency. Calcium intake may be low. Kidney function may be impaired, affecting how minerals are handled. Certain gastrointestinal conditions can limit absorption. Less commonly, endocrine disorders can alter PTH regulation.
That doesn’t mean fear—it means precision. The goal is to identify the true driver so the intervention matches the root cause. Otherwise, you may keep correcting one variable while another remains untreated.
After 40, the body’s feedback system may have multiple levers. A smart plan considers all of them.
A New Definition of Strength: Resilience Beyond Muscle
Bone health is not only a matter of preventing osteoporosis. It’s about preserving the skeleton’s capacity to remain structurally adaptive—capable of withstanding mechanical stress with less micro-damage accumulation and better mineralization quality.
When vitamin D and PTH are in a healthier alignment, the bone remodeling process can proceed with less unnecessary breakdown. That shift is quietly profound. It can influence long-term risk, mobility confidence, and the ability to maintain active years without constantly thinking about what might be deteriorating behind the scenes.
So the promise here is a perspective shift: you’re not merely trying to “take vitamin D.” You are helping your body speak a different hormonal language—one where bones are building rather than bargaining.





