
Vitamin D is one of those nutrients that quietly orchestrates a surprising number of body functions—bone remodeling, immune signaling, muscle performance, and even the cadence of cellular growth. Yet when people finally order a Vitamin D blood test, they often arrive at a single cliff edge: the number on the lab report. Two figures dominate conversations—30 ng/mL and 50 ng/mL. Which one is better? The answer is rarely binary. It depends on symptoms, health history, sun exposure, lab variability, seasonality, and the intended outcome. Let’s walk through the landscape with clarity, so the number becomes meaningful rather than mysterious.
Understanding the test: what “ng/mL” is really telling you
A vitamin D blood test usually measures 25-hydroxyvitamin D—the circulating metabolite that best reflects your vitamin stores. The unit ng/mL (nanograms per milliliter) helps clinicians estimate how much “reserve” your body has accumulated. This reserve is built slowly: from diet, supplements, and ultraviolet B exposure on the skin.
Because vitamin D behaves like a seasonal traveler, levels can drift through the year. Sunlight intensity, cloud cover, skin pigmentation, body mass, latitude, and sunscreen habits all influence the trajectory. So a single test is like taking a snapshot of a river’s flow—informative, but not the whole story.
It’s also worth remembering that laboratories may use different assay methods. That’s why one person’s “30” might correspond to a slightly different true value than another lab’s “30.” Small numeric differences can be noise, not a verdict.
30 ng/mL: where it lands on most reference ranges
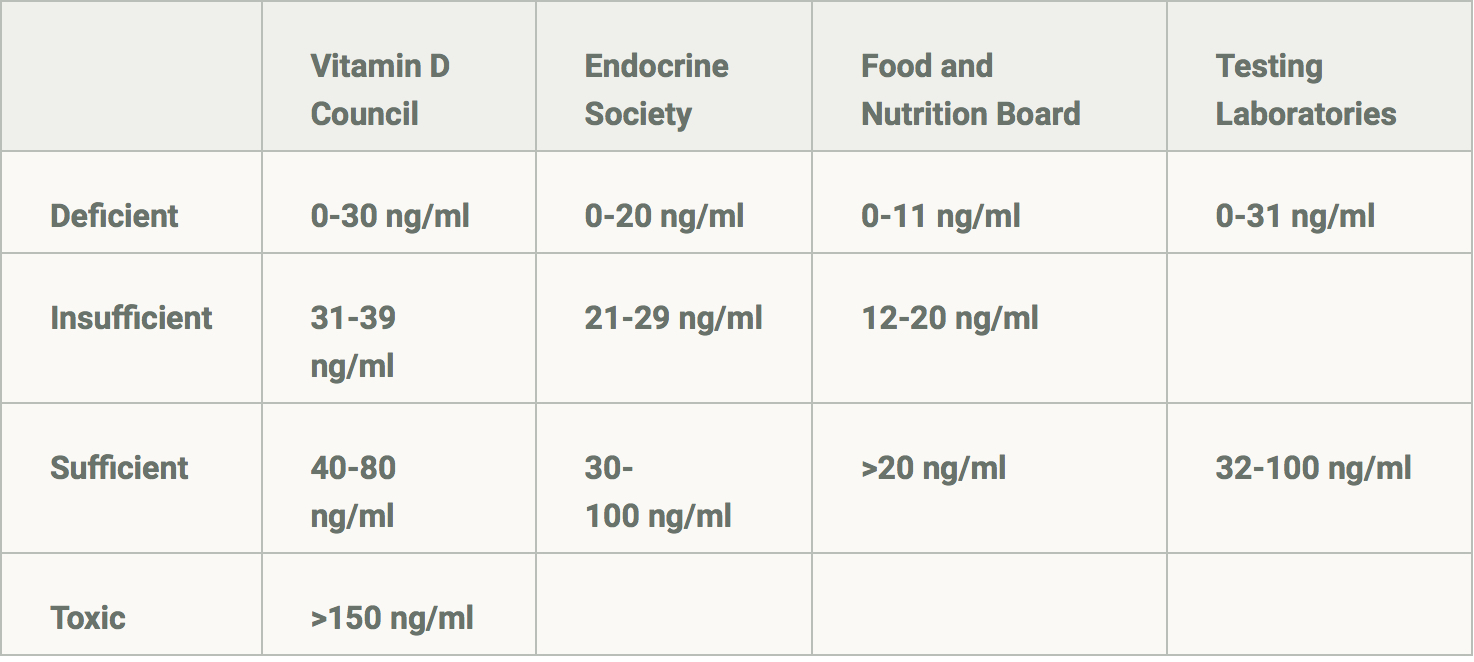
For many clinical guidelines, 30 ng/mL is treated as a practical threshold—often framed as the point where vitamin D status is no longer considered deficient for general skeletal health. In plain terms, 30 ng/mL usually indicates that the body has enough vitamin D to support typical bone metabolism and calcium handling.
However, 30 ng/mL can also sit in the “borderland” zone for people with higher demands—those with darker skin, malabsorption syndromes, chronic kidney concerns, osteoporosis risk, or limited sun exposure. In these scenarios, 30 may represent adequacy, but it might still feel like being at the minimum buoy rather than in the deeper waters.
Some readers interpret 30 ng/mL as “safe and done.” Others experience persistent symptoms—fatigue, muscle aches, or low mood—and wonder whether raising the number would bring relief. Sometimes it helps. Sometimes it doesn’t. Vitamin D is not a universal solvent; it’s more like a keystone. If other factors are driving symptoms, vitamin D alone won’t resolve the whole constellation.
50 ng/mL: the allure of “optimal” and what “better” could mean
50 ng/mL is frequently promoted as an “optimal” target, especially by wellness communities. The appeal is intuitive: if one number signals adequacy, then a higher number might signal resilience—more buffer for seasonal drops, more consistent support for musculoskeletal function, and potentially smoother immune modulation.
Yet the word “better” can mean different things depending on the goal. For bone health, the incremental benefit of rising from 30 to 50 is not guaranteed for everyone. For people with specific risk factors, a higher level may be more reliably protective. For others, the body’s response curve may flatten, and additional vitamin D may offer diminishing returns.
In nutrition science, it’s common to encounter a bell-shaped or plateau-like pattern—there is a point where more isn’t proportionally more effective. The question becomes: are you chasing a number, or are you solving a clinical problem?

Risk and restraint: the safety conversation beyond 50
Higher vitamin D levels aren’t automatically dangerous, but they deserve respect. The body can only convert so much vitamin D into useful forms, and excessive supplementation can elevate calcium levels in some circumstances. That can lead to symptoms such as nausea, constipation, excessive thirst, frequent urination, confusion, or in severe cases, kidney complications.
Most healthy individuals can reach mid-range targets with supervised dosing, but the safety equation depends on your baseline, your supplement regimen, your dietary calcium intake, and your medical context. If you’re already near 50 ng/mL, increasing further may be more about preference than physiology.
Think of vitamin D like a dimmer switch rather than a light switch. The aim is adequate illumination, not an over-bright glare.
Why 30 vs 50 can feel personal: symptoms, context, and variability
Some people feel better at 50; others feel unchanged. The difference often comes down to context. If you had low vitamin D, your body may be recalibrating systems that were under-supported. In such cases, moving from ~20 to ~35 can be dramatic, while moving from ~30 to ~50 may be subtle.
Conversely, if someone’s symptoms stem from anemia, thyroid imbalance, insufficient sleep, insufficient protein intake, or inflammatory conditions, a vitamin D increase won’t erase the underlying driver. Vitamin D is an important signal in immune and cellular pathways, but it doesn’t operate in isolation.
Also, consider absorption. People with malabsorption—celiac disease, inflammatory bowel conditions, bariatric surgery history, or certain medications—may struggle to maintain levels even with standard dosing. For them, 50 may require a different strategy than for someone who absorbs vitamin D effectively from diet and sunlight.
The “conversion” factor: ng/mL to nmol/L and why it matters
Lab reports may display vitamin D in different units. In some settings, results appear as nmol/L rather than ng/mL. A common conversion is roughly: 30 ng/mL ≈ 75 nmol/L and 50 ng/mL ≈ 125 nmol/L. This matters when comparing studies, guidelines, or discussions across countries.
Misreading units can lead to an incorrect interpretation—either underestimating a deficit or overestimating “optimal” levels. Always align units before making decisions about dosing.

How to decide: choosing the number based on goals
Rather than asking “Which is better?” ask “Better for what?” Here are practical goal-aligned perspectives:
Bone-focused maintenance: If your clinician is primarily concerned with skeletal health and you have no major risk factors, 30 ng/mL is often sufficient. The emphasis may shift to calcium intake, weight-bearing activity, and ensuring overall nutrition adequacy.
High-risk profiles: If you have osteoporosis risk, limited sun exposure, malabsorption, or specific chronic conditions, aiming closer to 40–50 may be reasonable, often with periodic monitoring to ensure stable levels.
Symptom-guided trials: Some people use a monitored vitamin D adjustment as an experiment. If symptoms improve with reaching a certain level—and other causes have been considered—that target becomes more meaningful.
Seasonal strategy: In winter months, levels may fall. In summer, they may rise. Some people stabilize around a mid-range like 40–50 to avoid dropping below a threshold in low-sun seasons.
In every case, the smartest plan is individualized dosing plus follow-up testing rather than blind chasing.
What readers can do next: interpreting your own lab report
If your result is around 30 ng/mL, consider asking: Do I have risk factors that make me more vulnerable to seasonal or physiological dips? Am I consistent with my supplement strategy (if any)? Do I have conditions or medications that affect absorption? Are my calcium and magnesium intake supportive?
If your result is around 50 ng/mL, consider whether the level is stable without aggressive dosing. Are you maintaining it with sensible intake? Do you have any conditions that warrant extra caution? Sometimes the “best” vitamin D level is the one you can sustain safely and consistently, not the one you can reach temporarily.
Finally, repeat testing can illuminate trends. A second measurement a few months later—after implementing a plan—often reveals more than the initial number alone.
A balanced conclusion: 30 vs 50, the realistic verdict
30 ng/mL often represents a meaningful baseline for vitamin D sufficiency, particularly for general bone metabolism. 50 ng/mL can be beneficial for certain people—especially those with risk factors, limited sun exposure, or malabsorption—where additional buffer may translate into more consistent physiological support.
But “better” is not inherently attached to the higher number. It’s attached to the body you’re working with, the symptoms you’re experiencing, the risks you carry, and the safety margins you respect. If 30 gets you stable and well, it may be the better target for you. If 50 brings steadier function and fewer symptoms under supervised care, it may be better than a minimalist threshold.
Ultimately, vitamin D isn’t a trophy. It’s a tool. The best result is the one that fits your health story—measured, monitored, and used with restraint.





