
Have you ever wondered why a number on a lab report—vitamin D—can seem to “pull levers” inside the body that regulate calcium so precisely? It’s a curious tango: vitamin D and parathyroid hormone (PTH) don’t merely coexist. They actively negotiate, often silently, to keep your calcium levels within an exquisitely narrow corridor. And here comes a playful challenge—what if your vitamin D is low, but your symptoms are oddly vague, as if your body is politely trying to compensate? That is where the link between vitamin D level and PTH becomes not just interesting, but consequential.
Vitamin D: the backstage architect of calcium absorption
Vitamin D is best understood as a prohormone-like coordinator that helps your intestine absorb calcium with efficient, almost architectural precision. When vitamin D levels are adequate, the gut can upregulate calcium transport machinery. The result is more calcium entering the bloodstream after meals, and that matters because calcium is not a “nice-to-have”—it’s required for muscle contraction, nerve signaling, and cellular signaling pathways that behave like finely tuned rhythm sections.
When vitamin D is insufficient, calcium absorption can wane. The body doesn’t like shortages. It responds with countermeasures—some immediate, some hormonal. One of the key hormonal responses involves the parathyroid glands and their messenger, PTH.
PTH: the emergency manager that protects calcium stability
PTH is released by the parathyroid glands, which function like vigilant sentinels. Their job is straightforward: maintain serum calcium. But the strategies PTH uses are not as simple as flipping a light switch. PTH influences multiple tissues.
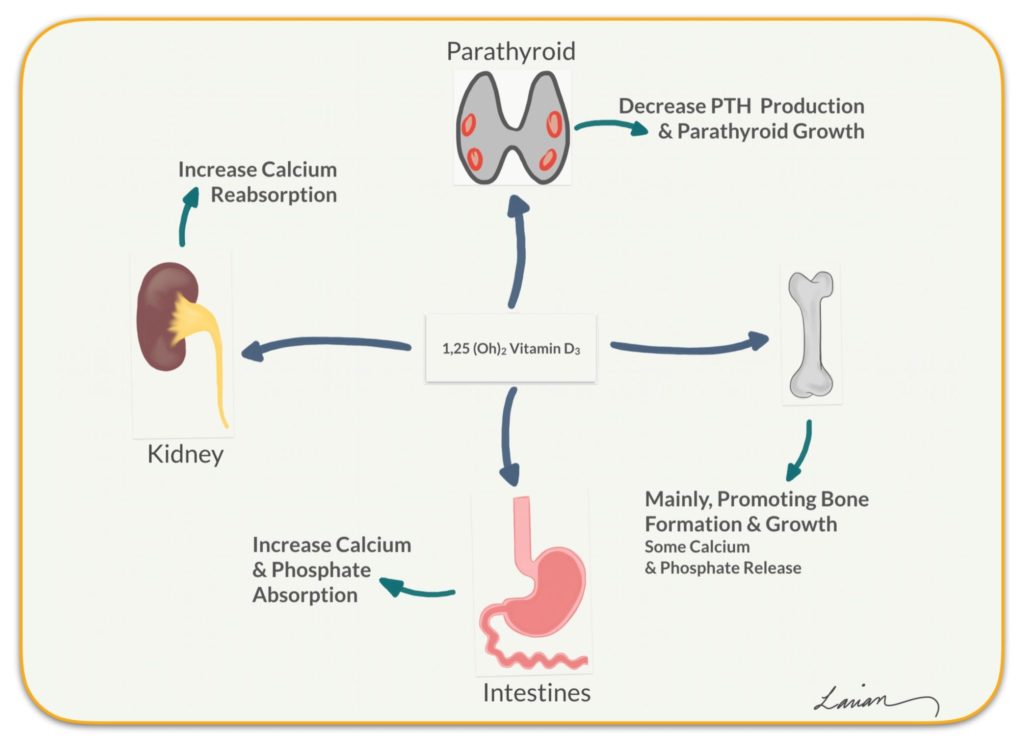
First, it nudges the kidneys to reduce calcium loss—helping keep calcium in the circulation. Second, it increases phosphate excretion, which can seem counterintuitive until you remember the broader goal: creating biochemical conditions favorable for calcium balance. Third, and most relevant to the vitamin D connection, PTH stimulates activation of vitamin D in the kidneys. That step helps create calcitriol (the active form of vitamin D), which then supports calcium absorption again.
In short, PTH is an adaptive regulator. When it rises, it often means the body is trying to correct a deficit in calcium availability—sometimes driven by low vitamin D.
The axis in motion: how vitamin D deficiency can drive PTH upward
Imagine calcium as a currency. Vitamin D helps you earn it from food. If vitamin D is low, your “income” drops. Then PTH steps in as a cost-saving executive: it conserves calcium, reallocates metabolic resources, and encourages the conversion of vitamin D into its active form.
This is why vitamin D deficiency is frequently associated with elevated PTH levels. The parathyroid glands detect calcium-related signals and respond by increasing PTH secretion—often before obvious symptoms appear. The pattern can resemble a subtle tug-of-war: vitamin D is insufficient, calcium absorption falters, calcium is perceived as borderline, and PTH rises to compensate.
However, compensation has a limit. Chronically elevated PTH may reflect a persistent supply problem—one that vitamin D replenishment may help address.

Vitamin D status: why the “label” matters—25(OH)D versus active vitamin D
Not all vitamin D measurements are equal. Clinicians commonly assess 25-hydroxyvitamin D, often written as 25(OH)D, because it reflects overall vitamin D stores more reliably than the active hormone form. Active vitamin D (calcitriol) is tightly regulated by the body and can vary based on kidney function and PTH activity.
So, if you’re studying the link between vitamin D and PTH, 25(OH)D is frequently the more informative “starting point.” When 25(OH)D is low, it can foreshadow elevated PTH as the body attempts to sustain calcium balance.
A short sentence with a long implication: the wrong lab marker can blur the story. Using the appropriate measure helps clarify whether the parathyroid response is likely secondary to vitamin D insufficiency—or whether other causes are involved.
What counts as a potential complication? Secondary hyperparathyroidism
When PTH rises because of an external or secondary driver—such as vitamin D deficiency—this is often described as secondary hyperparathyroidism. The adjective “secondary” is important; it implies the parathyroid glands are responding, not malfunctioning in isolation.
In many individuals, correcting vitamin D improves PTH levels over time. But if PTH remains stubbornly elevated, other factors may be at play. Chronic kidney disease can reduce the ability to activate vitamin D. Malabsorption syndromes can prevent vitamin D absorption even when intake seems adequate. Certain medications may alter vitamin D metabolism. Each scenario can produce a similar hormonal signature: PTH up, sometimes calcium normal, sometimes calcium borderline.
That’s the challenge hidden in plain sight—two people can have the same PTH level, yet their underlying narratives may be completely different.
Calcium isn’t always low: the quiet difference between serum calcium and demand
Here’s a twist that often surprises people. With vitamin D deficiency, serum calcium can be normal for a period while PTH rises. The body may maintain blood calcium by borrowing from other reserves, enhancing kidney conservation, and increasing calcitriol production.
Yet “normal” calcium doesn’t always mean “optimal physiology.” Bone may be paying a hidden price if calcium balance is sustained through skeletal contributions. PTH can influence bone remodeling, shifting the balance between bone formation and resorption. Over time, this can affect bone mineral density and increase fragility risk.
So a lab value can look calm while the internal dynamics are anything but calm.
Bone and muscle: downstream effects of chronically elevated PTH
Bone is a dynamic tissue, always remodeling. Persistent PTH elevation—especially when driven by chronic vitamin D insufficiency—can tilt remodeling toward bone breakdown. The magnitude of impact varies, but the direction is clinically meaningful. Reduced bone mineral density can raise fracture susceptibility, particularly in older adults or those with additional risk factors.
Muscle function may also feel the consequences indirectly. If vitamin D deficiency contributes to calcium and phosphate dysregulation, muscle performance can suffer. The symptoms may be nonspecific: weakness, aches, or a sense of sluggishness. Sometimes it’s not dramatic. Sometimes it’s simply “off.”
A playful question lingers here: if your muscles feel less reliable, could your calcium economy be under hormonal strain?
How clinicians connect the dots: patterns and correlations
Rather than chasing a single number, clinicians often interpret the relationship between 25(OH)D and PTH. A common pattern is an inverse relationship—lower vitamin D tends to accompany higher PTH. But medical reality is rarely a straight line. Individual physiology, baseline calcium intake, sun exposure, renal function, and magnesium status can all influence the axis.
Magnesium deserves mention because it can affect parathyroid function and vitamin D metabolism. If magnesium is low, PTH regulation may become less efficient. Phosphate handling also matters; PTH reduces serum phosphate, and altered phosphate balance can influence calcitriol activity.
So the link between vitamin D and PTH isn’t just a single conversation—it’s a multi-threaded discussion among minerals, organs, and hormones.
Therapeutic implications: addressing vitamin D to potentially normalize PTH
When vitamin D deficiency is the probable driver, replenishing vitamin D is often a logical first step. As vitamin D stores rise, intestinal calcium absorption may improve, reducing the parathyroid “signal” that calcium needs emergency management. Over weeks to months, PTH may decrease, sometimes dramatically, sometimes modestly.
But dosing is not one-size-fits-all. Higher-risk individuals—such as those with malabsorption, chronic kidney disease, or significant baseline deficiency—may require tailored regimens. Additionally, calcium intake should be assessed. If vitamin D is supplied without adequate dietary calcium, the body’s demand may not fully resolve.
The goal is not merely to drive PTH down. The goal is to reestablish biochemical harmony—less hormonal urgency, improved calcium absorption, and preserved skeletal integrity.
A final perspective: treat the pattern, not just the number
The link between vitamin D level and PTH is ultimately a story about regulation under pressure. Vitamin D supports calcium absorption; PTH protects calcium stability. When vitamin D runs low, PTH frequently rises as compensation—sometimes silently, sometimes with downstream consequences for bone and muscle.
And now the closing challenge: before dismissing a borderline lab result as “not serious,” ask what story the body is telling with its hormones. A thoughtful interpretation—considering vitamin D status, calcium trends, kidney function, and mineral balance—turns scattered numbers into a coherent narrative. That’s where the science becomes personal, and where prevention becomes possible.





