There’s a particular moment most people recognize: a blood test result arrives, and suddenly a simple vitamin becomes a passport to a whole universe of questions. “How low is low?” “Do I need a prescription?” “Is this serious, or just a temporary inconvenience?” It feels oddly personal—like Vitamin D is either quietly working in the background or quietly failing, depending on one number. That common observation is familiar, yet it’s also the doorway to deeper fascination. Because vitamin D treatment isn’t only about deficiency; it’s about biology’s fine-grained bookkeeping, the body’s varying thresholds, and the physician’s balancing act between replenishment and safety.
The number on the lab report: where “normal” stops and “action” begins
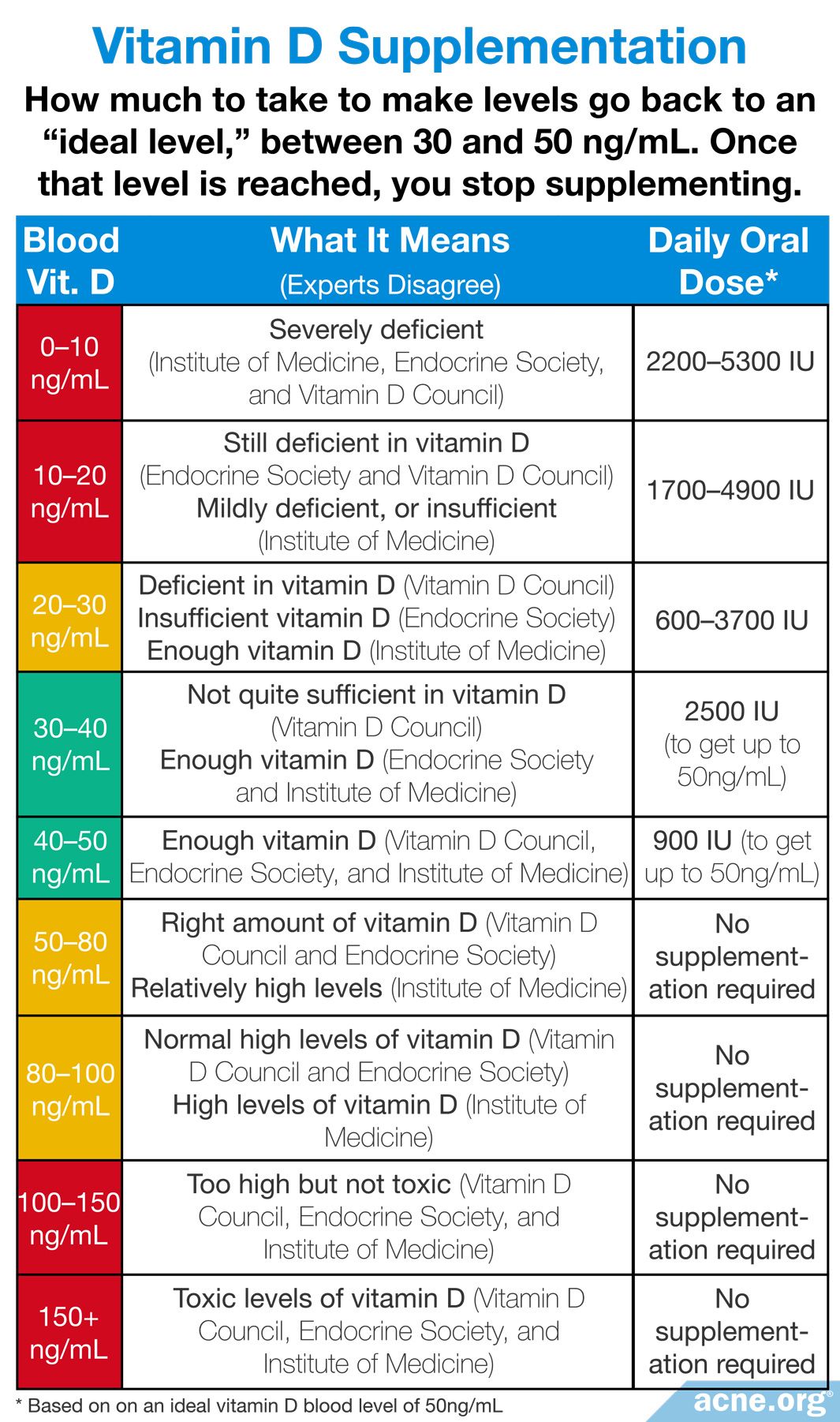
When people ask what level of Vitamin D requires prescription treatment, they usually start with the same anchor: the serum 25-hydroxyvitamin D measurement. This metabolite is considered the best snapshot of vitamin D status. But “requiring prescription” isn’t governed by one universal instinct. It’s influenced by severity, symptoms, comorbidities, and risk of complications.
In broad strokes, many clinical frameworks treat severe deficiency as a more urgent situation. Mild insufficiency is often managed with lifestyle changes and over-the-counter supplementation. Moderate deficiency may be treated with higher-dose oral regimens, sometimes using non-prescription products, depending on local practice and the clinician’s preference. Prescription therapy tends to appear when levels are markedly low, when rapid correction is desirable, or when standard dosing hasn’t worked.
What makes this topic subtly captivating is that the lab number can feel absolute, yet human physiology is anything but. Two people can share a similar result and have different needs due to absorption, body mass, liver handling, and the speed at which their levels fall again.
When prescription treatment becomes likely: severity and clinical context
Prescription vitamin D is commonly considered when deficiency is profound—especially levels that suggest a meaningful depletion of stores. The rationale is pragmatic: a more intensive regimen can replenish reserves faster, reducing the period of biochemical vulnerability. Yet severity isn’t the only trigger. Physicians also look at the “story behind the number.”
Several contextual clues often push management toward prescription dosing: persistent low levels despite adherence, malabsorption syndromes, chronic kidney disease, medications that interfere with vitamin D metabolism (such as certain anticonvulsants), and conditions that increase calcium demand. Symptoms matter too—muscle weakness, bone pain, fatigue that won’t settle, or signs suggestive of osteomalacia. In these cases, clinicians are not merely aiming for a “target range.” They’re trying to stop a cascade.
Sometimes the deeper reason for fascination is that vitamin D behaves like a hormone with a long echo. Its effects ripple through calcium balance, bone remodeling, immune signaling, and cellular regulation. When the deficiency is severe, that echo can become loud enough to disturb daily life.
Mild deficiency vs. severe deficiency: why the treatment threshold isn’t just arithmetic
It’s tempting to imagine a simple rule: below a certain value, use prescription doses; above it, use supplements. Real medicine is more textured than that. Vitamin D thresholds are often interpreted alongside other labs, especially calcium, parathyroid hormone (PTH), and sometimes phosphate. If PTH is elevated, the body may be compensating by pulling calcium from bone—an indication that deficiency is affecting more than skin-level status.
This is where the “common observation” becomes a deeper question: why does the same vitamin concentration matter so much? The answer lies in regulation. When vitamin D is inadequate, absorption of calcium decreases. The parathyroid glands react, trying to maintain blood calcium stability. That compensation is effective short-term, but it can have long-term consequences for skeletal integrity. Prescription regimens may be favored when the physiological compensation looks active.
So, the threshold for prescription treatment isn’t only about the measured number. It’s also about what the body is doing in response to that number.
Common prescription strategies: daily, weekly, and “repletion then maintenance”
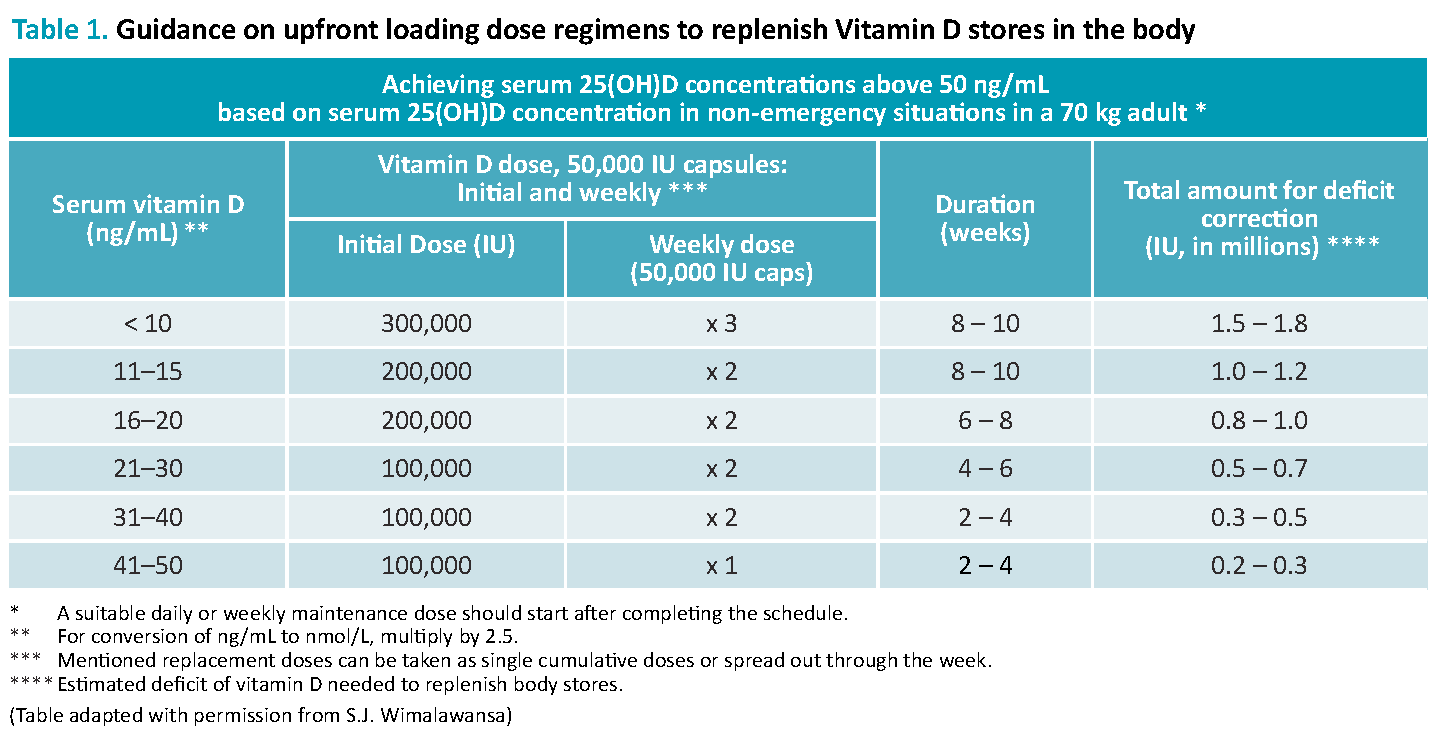
Prescription treatment often follows a recognizable choreography: repletion first, then maintenance. The goal during repletion is to restore levels quickly enough to correct deficiency-related physiology. Maintenance dosing is designed to sustain that improvement without overshooting.
There are typical patterns clinicians may use. Some protocols rely on high-dose daily therapy for a defined period. Others use weekly or intermittent regimens that deliver a larger dose per administration. The specific choice depends on patient preference, adherence likelihood, risk profile, and the clinician’s interpretation of severity.
Adherence is not a minor detail here; it’s a cornerstone. People sometimes start supplements enthusiastically and then drift. When a deficiency is driving symptoms or biochemical compensation, drifting can prolong the problem. Prescription regimens can reduce the frequency of decision-making, making them easier to follow—and easier for clinicians to evaluate for response.
Safety and the “too much” concern: why prescription doesn’t mean reckless
Prescription vitamin D exists because correction sometimes requires intensity. But intensity invites a second question: how do clinicians prevent toxicity? They don’t just prescribe and hope. They monitor risk factors and may check follow-up labs.
Excessive vitamin D can increase calcium absorption, potentially leading to hypercalcemia. That can cause symptoms such as nausea, constipation, confusion, excessive thirst, and frequent urination. Most cases of toxicity relate to excessive dosing or unusual sensitivity. Still, the concern is real enough that clinicians prefer structured regimens and follow-up—especially in people with kidney disease, granulomatous conditions, or certain medication combinations.
Even the fascinating parts of vitamin D—its broad biological reach—come with responsibility. Prescription care is often a way to make replenishment precise, not merely powerful.
Why some people need more than others: absorption, body composition, and metabolism
Two individuals with similar intake can have very different serum levels. This is one of the deeper reasons vitamin D remains such a perennial obsession in health discussions. Body composition can influence vitamin D distribution. Heavier adiposity may sequester vitamin D in fat tissue, effectively reducing the circulating fraction.
Absorption also plays a major role. Gastrointestinal issues—celiac disease, Crohn’s disease, inflammatory bowel patterns, prior bariatric surgery, and pancreatic insufficiency—can reduce uptake. Liver disorders can impair conversion steps that activate vitamin D metabolites. Kidney disease can affect how the final active forms are handled. In these situations, a “standard” supplement dose can feel like throwing water into a leaky bucket.
That’s why prescription treatment sometimes appears not because the person is “noncompliant,” but because physiology requires a different strategy.
Special populations: pregnancy, older adults, and chronic disease
Prescription thresholds can shift in special populations. Older adults often produce less vitamin D in the skin and may absorb it less efficiently. Bone health is also more fragile. For pregnancy and breastfeeding, clinicians consider the balance of maternal stores and fetal/infant needs, selecting dosing to support safe physiology.
Chronic diseases can complicate interpretation. Kidney impairment may reduce conversion of vitamin D metabolites. Certain endocrine disorders and medications can alter vitamin D metabolism. The same number on a lab result can mean different degrees of functional deficiency depending on the underlying condition.
In these populations, “prescription treatment” is frequently less about strict thresholds and more about preventing complications with a predictable plan.
Follow-up testing: what success actually looks like
After a prescription course, clinicians may recheck vitamin D levels and sometimes calcium, depending on risk. Success is not only reaching a target concentration; it’s normalizing the body’s internal signals. If PTH has been elevated, the correction should accompany improvement in bone-related chemistry.
There’s also an important psychological dimension. People sometimes expect vitamin D to behave like a quick-fix medication. But vitamin D is more like a slow-building reservoir. The body’s remodeling processes and metabolic adjustments take time. That’s why repletion regimens are paired with maintenance strategies—so the gains don’t vanish after the initial enthusiasm fades.
A cohesive plan makes the entire process feel less mysterious. The fascination remains, but it becomes structured rather than chaotic.
What to do next: translating “low” into a safe, individualized plan
If your 25-hydroxyvitamin D level suggests deficiency, the next step is not simply choosing a dose from a chart. It’s a conversation that includes symptoms, medical history, concurrent lab results, diet, medication profile, and absorption risks. Prescription therapy may be appropriate when deficiency is severe, when symptoms or biochemical compensation are present, or when standard dosing has failed.
At the same time, “prescription” should not be interpreted as a guarantee of speed or certainty. It’s an instrument for more controlled correction and monitoring. It’s medicine’s way of acknowledging that the body’s thresholds are personal—and that the safest correction is rarely a one-size number.
If you want to understand whether prescription treatment is warranted for your situation, ask your clinician how severity, risk factors, and follow-up testing fit together. That question transforms a lab report into a roadmap, and it turns uncertainty into a plan you can actually follow.