
Alternating vitamin D doses sounds deceptively simple: take a modest amount one day, a higher amount the next, and assume your body will “average out” the total. Yet vitamin D metabolism isn’t a casual ledger. It is a slow-moving biochemical process, influenced by absorption, body stores, kidney function, skin physiology, and even how consistently the habit is maintained. If you’re asking whether you can alternate “2000 IU one day” with “5000 IU the next,” the real answer depends less on the numbers on the label and more on your baseline vitamin D status, your risk profile, and the purpose of the supplementation.
What “alternating doses” actually means in the body
When people alternate doses, they often imagine a neat swing between two levels—like a pendulum. In practice, vitamin D behaves more like a long-duration reservoir. After ingestion, vitamin D is converted in stages to its active forms and stored in fat and other tissues. Because of this storage, blood levels don’t leap dramatically overnight. They rise gradually, then flatten, and may remain relatively stable even when day-to-day dosing changes.
However, this doesn’t mean alternating is automatically equivalent to steady dosing. Blood concentrations can still drift upward or downward depending on the starting point. A person with low vitamin D may respond more noticeably to higher intermittent doses, while someone already replete may experience a slower—and sometimes unnecessary—overcorrection. The body rarely treats supplemental timing as a mere scheduling trick.
2000 IU one day and 5000 IU the next: is it reasonable?
Let’s consider the arithmetic first. Alternating 2000 IU and 5000 IU produces an average of 3500 IU per day across a two-day cycle. Whether that average is appropriate depends on what “appropriate” means for your goals: maintenance, repletion, or treatment of deficiency.
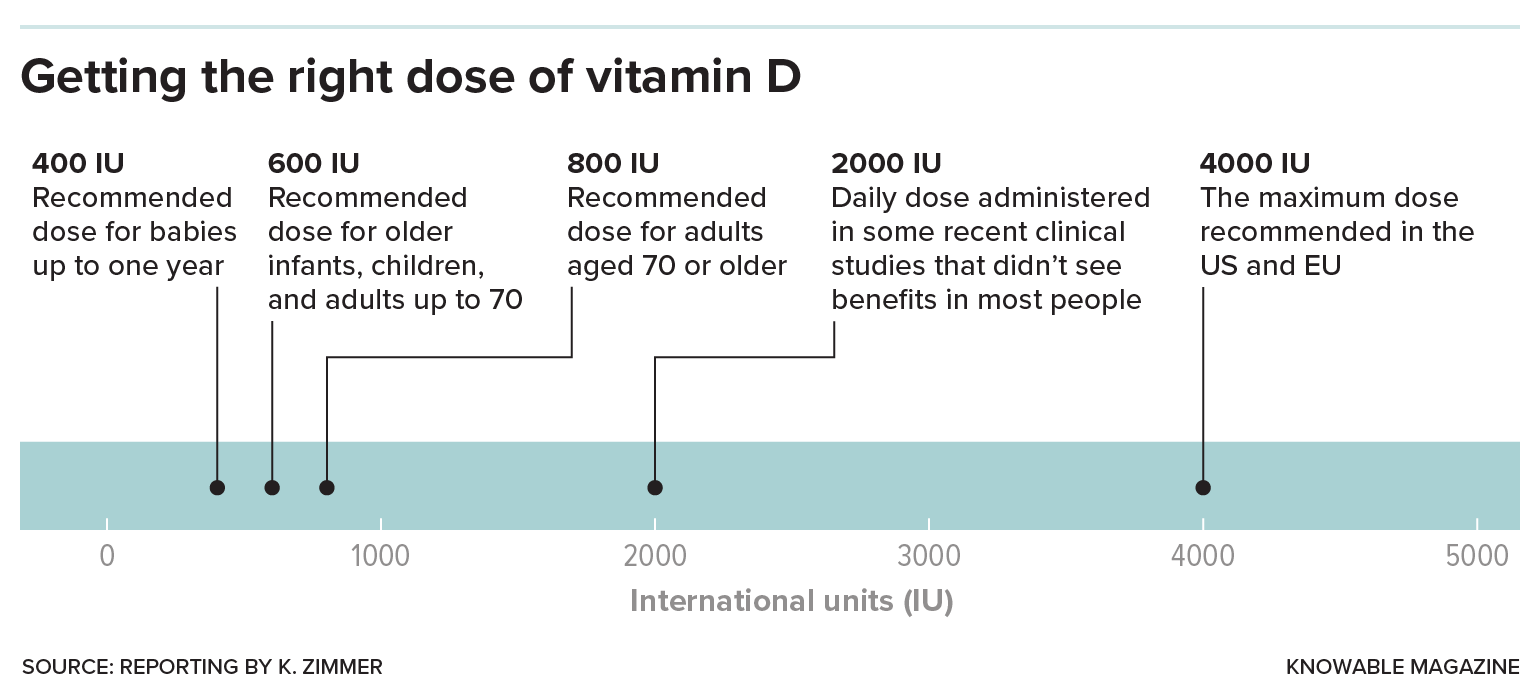
For many adults, daily maintenance regimens often fall in the vicinity of 600–2000 IU, though some clinicians prescribe higher amounts when levels are low. The frequently cited upper safe limit for routine daily intake is typically 4000 IU for adults, but exceptions exist under medical supervision, especially when deficiencies are confirmed via blood testing.
Here’s the crux: alternating schedules may keep average intake within a tolerable range while still delivering occasional peaks. Peaks matter less for most people than total exposure over time, but in sensitive individuals—such as those with certain medical conditions—peaks can contribute to a cumulative risk pattern. The safest approach is not to rely solely on the average, but to pair the plan with a measured baseline and follow-up testing.
The difference between “safe for you” and “safe in general”
Vitamin D safety is not one-size-fits-all. Some risk factors elevate concern even when doses appear “moderate.” Examples include a history of kidney stones, chronic kidney disease, hyperparathyroidism, granulomatous diseases (like sarcoidosis), or disorders that increase calcium absorption. In these cases, higher or uneven dosing could raise calcium levels more than expected.
Body size also matters. Two people taking the same IU dose can experience different serum changes due to differences in adiposity and vitamin D distribution. Genetic variations in vitamin D binding proteins can shift how much becomes bioavailable. In other words, your biochemistry is not a universal calculator—it’s a customized ecosystem.
Daily consistency vs. alternating patterns
Alternating doses may be more about convenience than physiology. Many people choose it because they forget one day, want to “boost” every other day, or prefer a schedule that feels psychologically manageable. From a purely practical standpoint, vitamin D’s half-life is long enough that occasional variations are unlikely to cause sudden harm in healthy individuals.
Still, consistency has advantages. Steady dosing tends to produce smoother serum levels, which can be beneficial if you are already near the upper end of optimal range. Alternating can be fine, but it introduces a minor wobble that you may not notice until you check lab results—especially if you are stacking vitamin D with other supplements.
Short sentence: Labs tell the truth more reliably than intuition.
Long sentence: If your goal is to correct deficiency, your doctor may prefer a clearly defined regimen (either daily or weekly) and then retest, rather than improvising on a day-to-day basis.
Why testing matters: what labs to consider
If you’re contemplating alternating 2000 IU and 5000 IU, it’s wise to measure your current status. The primary marker is typically 25-hydroxyvitamin D, sometimes accompanied by serum calcium. In certain cases, clinicians also assess parathyroid hormone (PTH) or markers of kidney function.
Here’s how testing reshapes decisions. If your level is clearly deficient, higher short-term dosing is often used to “recharge the depot,” then stepped down for maintenance. If your level is already sufficient, maintaining with a lower and more stable dose may be the more judicious path. If your level is borderline and you’re alternating high doses, you may overshoot slowly without realizing it.
Timing matters too. Retesting is often considered after a few months, since vitamin D repletion is gradual. Trying to optimize too quickly can lead to unnecessary adjustments and confusion.
Potential downsides of higher intermittent dosing
Most people tolerate vitamin D supplementation well, but the concern isn’t usually the dose you took yesterday—it’s the cumulative effect over time. Excess vitamin D can increase calcium absorption, potentially leading to hypercalcemia. Symptoms may include nausea, constipation, unusual thirst, frequent urination, confusion, and fatigue. Kidney stones can be a particular hazard in susceptible individuals.
Not everyone experiences symptoms, which is why lab monitoring becomes especially important when dosing climbs or when there are risk factors. Some supplements also contain calcium. If you take vitamin D and calcium together, your risk profile changes significantly, and your body may respond differently than expected.
Another hidden variable: sunlight. If you’re also getting substantial sun exposure, the effective “total dose” may be higher than you think. Alternating schedules can unintentionally stack with environmental vitamin D production.
How long should you alternate?
Alternation is usually best viewed as a phase, not a lifestyle sentence. If you are repleting deficiency, your regimen may be temporary—followed by a maintenance dose once your labs normalize. If you’re maintaining sufficiency, a simpler schedule often suffices.
Longer alternation without reassessment can lead to dose creep: you may start at 2000/5000 IU because it feels reasonable, then forget to revisit the plan. Over months, that can nudge levels upward. The remedy is not fear; it’s periodic review.
Different content readers can expect: practical scenarios
Readers typically fall into a few narrative categories, and each one benefits from a different kind of guidance. One group is “the newly concerned” reader—someone who saw a low vitamin D result and wants a concrete plan. Another is “the busy optimizer”—someone who wants an easy schedule that doesn’t require daily memory. A third is “the risk-aware reader”—someone with kidney history, autoimmune granulomatous conditions, or concurrent supplement use.
Expect content to address each scenario with nuance: what to ask your clinician, what lab changes mean, how to interpret symptoms, and how to avoid supplement stacking. A professional article should also include plain-language safety thresholds and clarify that IU amounts are not the only variable—baseline level, comorbidities, and calcium intake can matter just as much.
Practical tips if you choose to alternate
If you and your clinician decide alternating is appropriate, treat it like a controlled experiment. Keep the regimen consistent for a defined period. Avoid adding extra vitamin D from multiple products. Check the full label of all supplements, including multivitamins and “immune support” blends.
Pair supplementation with responsible habits: maintain hydration if you have a kidney stone history (as advised), and consider dietary calcium strategically rather than impulsively. Also remember that vitamin D is fat-soluble, so absorption is often better with a meal containing some dietary fat.
The bottom line: when alternating is a sensible choice vs. a gamble
Alternating 2000 IU one day and 5000 IU the next averages to 3500 IU per day, which may be reasonable for some people under supervision—especially if correcting low levels. It is less certain for someone with already-sufficient vitamin D, high calcium intake, kidney vulnerabilities, or conditions that elevate calcium absorption. The most responsible approach is to anchor any dosing plan to baseline labs, clarify goals, and reassess after an appropriate interval.
Short sentence: Your blood levels should guide your schedule.
Long sentence: If the regimen is tailored to your situation and monitored thoughtfully, alternating can be a workable strategy rather than a reckless improvisation.



