Vitamin D is one of those quiet nutrients that seems to do everything—supporting bone mineralization, modulating immune signaling, and nudging hundreds of cellular processes toward equilibrium. Yet when people ask, “What’s the difference between Vitamin D3 sulfate from the sun versus oral D3?” the conversation shifts from simple supplementation to a more intricate story about chemistry, skin biology, and how the body decides what to keep, convert, or circulate.
Setting the Stage: Vitamin D3, Sulfate, and the Body’s Sorting System
To understand the comparison, it helps to imagine the body as an efficient customs office. Vitamin D3 (cholecalciferol) is a precursor—useful, but not always the final form the body wants. After exposure to sunlight or ingestion, vitamin D must undergo biochemical “processing” so it can participate in downstream pathways.
Sulfate appears in this story because the body commonly uses sulfate groups as chemical tags. These tags can alter solubility, stability, transport behavior, and the kinetics of how molecules travel through tissues. In certain contexts, vitamin D metabolites may appear with sulfate modifications, reflecting the body’s adaptive chemistry. The sun is not merely a light source; it can trigger a cascade that influences which metabolites are generated in the first place, and how they are handled afterward.
Oral D3, by contrast, is usually delivered as cholecalciferol. From there, the body processes it through its own conversion routes. The “difference” is not just where vitamin D starts—it’s also what the body encounters during the transition from precursor to active signaling molecules.
From Sunlight to Skin: What Happens Before Vitamin D Enters the System
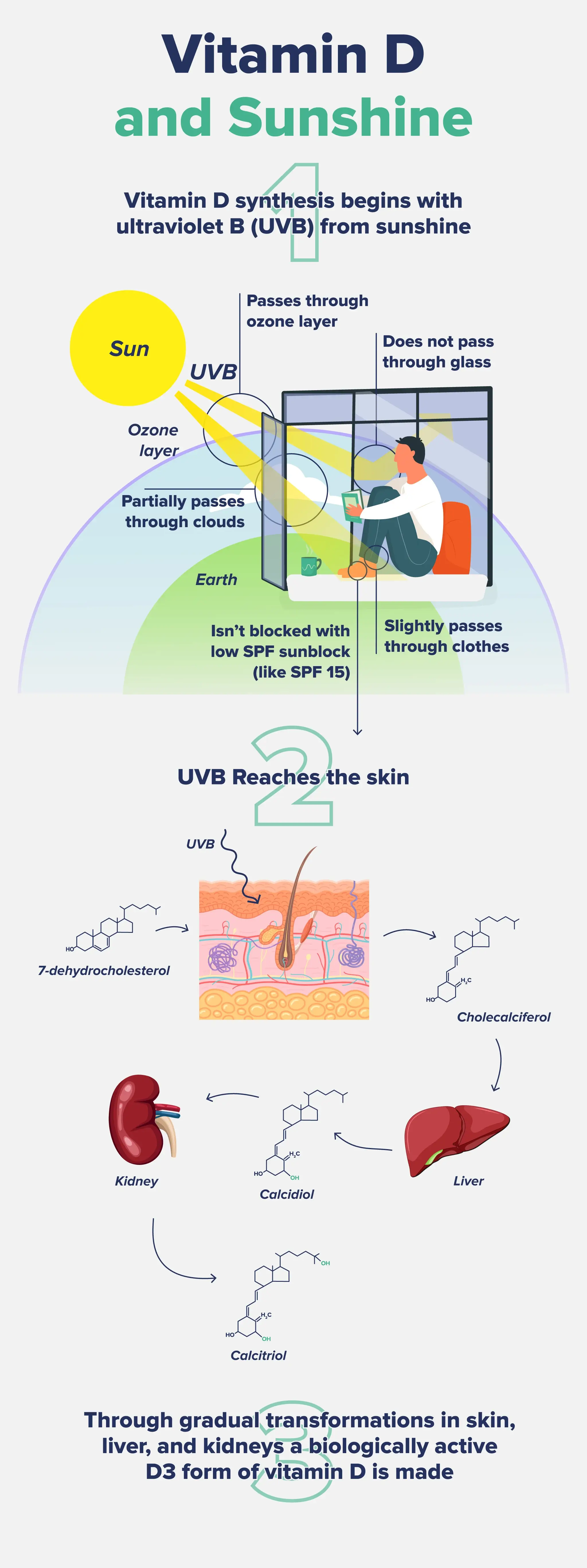
Sunlight—specifically ultraviolet B (UVB)—acts like a biochemical switch in the skin. Under the right conditions, UVB converts a cholesterol-like compound into pre–vitamin D3, which then thermally isomerizes into vitamin D3. This sequence is remarkably elegant. It is fast, localized, and influenced by several variables.
Skin tone, season, latitude, cloud cover, time of day, and even sunscreen use can shift the amount of vitamin D3 formed. Clothing coverage also changes exposure geometry. There’s a reason two people can live in the same city and have very different vitamin D status.
Now consider the “sulfate” element. In the skin and in the circulation, metabolites can be modified by conjugation pathways. Sulfation is one such modification. It can influence how metabolites move through the aqueous environment of blood and how long particular forms persist.
Key expectation: sun-derived vitamin D metabolites may include a blend of related forms, and some may carry sulfate groups due to the body’s ongoing conjugation and transport mechanisms.
Oral D3: A Direct Route Through Digestion and Liver-Orchestrated Metabolism
Oral vitamin D3 is absorbed through the digestive tract, often with the help of bile salts and dietary fat. That means meal composition can matter. A dose taken with a low-fat meal may absorb less efficiently than one taken with adequate dietary lipids.
Once absorbed, vitamin D3 enters circulation and is transported to the liver for major transformations. The liver typically converts vitamin D3 into a circulating intermediate that reflects body stores and is often used as a marker in clinical testing.
Oral D3 generally aims to increase vitamin D status by supplying a precursor in a controlled dose. It’s less dependent on daylight conditions and more predictable for many people—especially those in higher latitudes, those with limited outdoor exposure, or those with occupational constraints.
Key expectation: oral D3 largely delivers the parent molecule, and the body then performs conversion steps, rather than relying on skin photochemistry to begin the process.
What “Vitamin D3 Sulfate” Might Mean in Practice
In everyday nutrition talk, “vitamin D3 sulfate” can sound like a single, universally defined supplement form. In reality, sulfate modifications refer to a chemical pattern—adding a sulfate group to a vitamin D–related molecule. Whether and how much sulfate-conjugated vitamin D is produced can depend on tissue-specific enzyme activity and the timing of metabolism.
Some people assume sulfate-conjugation automatically means “better” or “stronger.” That assumption is too simplistic. Sulfation can be a means of tuning pharmacokinetics—altering how metabolites distribute, resist degradation, and interact with receptors indirectly. In other words, sulfate tags may not reflect ultimate biological potency; they often reflect transport and processing behavior.
Think of it like language translation. The body may convert vitamin D into different “dialects” depending on where it needs the message delivered.
Absorption Efficiency: Sunlight Isn’t a Supplement, and Supplements Aren’t Sun
Sun exposure can generate vitamin D3 without requiring digestion, but it is constrained by environmental factors. Your skin must do the chemistry, and your ability to absorb sunlight varies with lifestyle and biology.
Oral D3, meanwhile, is limited by gastrointestinal absorption and metabolic handling. Absorption can be influenced by age, gut health, bile production, and concurrent medications. Some conditions can reduce absorption, while others have less effect.
The practical difference is predictability. Oral dosing tends to be consistent in the amount provided. Sunlight exposure tends to be variable, sometimes dramatically.
Bioavailability and Metabolic Pathways: Timing, Conversion, and “Residence Time”
Both sun-derived and oral vitamin D3 ultimately rely on conversion pathways to support active biological functions. The divergence lies in the initial distribution of forms and how long certain metabolites remain detectable.
Sulfate-conjugated forms can have different “residence time” in circulation compared with non-conjugated precursors. Residence time affects how the body’s downstream systems see vitamin D signals over hours and days. Long story short: the same overall vitamin D status can emerge through different biochemical trajectories.
Oral D3 often increases circulating intermediates that reflect stored vitamin D. Sunlight can also raise those intermediates, but the distribution of transient metabolites may differ in ways that lab tests may or may not capture depending on what’s measured.
Clinical Markers: How Testing Shapes What You Think You’re Getting
Most standard assessments focus on vitamin D status using commonly reported markers that represent storage and recent changes. However, sulfate-conjugated metabolites are not always part of routine panels. That means people can feel confident about “having vitamin D,” while the specific metabolite profile remains unknown.
Interpreting results becomes a narrative exercise. A lab value might improve after sun or oral supplementation, yet the underlying metabolite choreography could differ. Some people also experience variability in response despite similar lab changes, suggesting that tissue-level handling and receptor sensitivity matter.
Key expectation: standard tests may not distinguish “sulfate signature” differences, so outcomes can be inferred only indirectly through trends and symptoms.
Safety and Risk: Dose Control Versus Exposure Uncertainty
Sunlight has a safety feature: the body tends to limit excessive vitamin D production through feedback mechanisms in the skin and photodegradation pathways. However, that does not mean sun exposure is risk-free. Skin cancer risk, photoaging, and eye damage remain real concerns.
Oral D3 has a different safety profile. It is dose-controlled, but overdosing can raise levels too high if dosing exceeds individual needs. People sometimes stack products unintentionally—multivitamins, calcium blends, and separate D3 capsules—creating a hidden total dose.
When comparing sun-derived sulfate-conjugated metabolites to oral D3, remember this: safety is not only chemistry. It’s also behavior, dosing discipline, and long-term exposure patterns.
Different Types of Content Readers Can Expect: Practical Guidance, Chemistry, and Real-World Scenarios
Articles on this topic typically fall into three content lanes, and a comprehensive understanding blends all three. First, there’s the practical lane: how to get vitamin D safely, when to consider supplements, and how to interpret lab work. Short checklists and dosing examples often live here, along with lifestyle adjustments like safe outdoor scheduling and meal timing.
Second, there’s the chemistry lane. This is where sulfate conjugation, metabolite forms, and conversion pathways appear. Expect longer paragraphs, more technical descriptors, and conceptual metaphors that translate enzyme behavior into something your mind can hold.
Third, there’s the lived-experience lane. This includes scenarios: someone living in a northern climate, a person with limited mobility, an athlete training indoors, or a caregiver managing a household. These stories often highlight why “sun versus oral” is really “your reality versus the idealized plan.”
The richest content connects these lanes. It doesn’t just list facts. It shows how they interact—how the chemistry influences markers, how markers influence decisions, and how decisions influence outcomes.
Choosing the Better Approach: Matching Vitamin D Strategy to Your Life
If your schedule allows meaningful, safe sun exposure, sunlight can be a natural way to support vitamin D3 production while also benefiting circadian cues and mood—though those effects are separate from vitamin D metabolism.
If sunlight is inconsistent or risk-averse behavior dominates, oral D3 offers control and convenience. Many people prefer it because dosing can be tailored, and absorption can be supported by taking it with appropriate dietary fat. It also fits well for those with darker skin tones, older age, or indoor-centric lifestyles where UVB exposure is limited.
For some readers, the best answer may be hybrid: safe outdoor exposure when feasible plus targeted oral supplementation when needed. The goal is not to “win” a chemistry contest between sun and capsules. The goal is to maintain healthy vitamin D status while minimizing risk and maximizing adherence.
The Bottom Line: It’s Not Just Vitamin D3—It’s the Metabolite Journey
The difference between Vitamin D3 sulfate from sun and oral D3 is best understood as a difference in starting conditions and biochemical travel routes. Sunlight initiates skin-based photochemistry and may involve sulfate-conjugated metabolites along the way. Oral D3 delivers the precursor through digestion and steers it through the body’s conversion pathways in a more dose-predictable manner.
Both strategies can support vitamin D status, but the “how” may vary—especially in metabolite profiles that routine testing might not capture. Ultimately, the most effective choice respects your environment, your health context, and your ability to follow through consistently.