Have you ever wondered why your body treats calcium like it’s in a high-stakes juggling act—while vitamin D quietly adjusts the spotlight from the background? Now picture this: parathyroid hormone (PTH) is the ringmaster, stepping in whenever the calcium levels drift off-script. But here’s the playful twist—what if the ringmaster is doing its job perfectly, yet the stage still looks wrong? That “almost right” feeling often comes from a subtle challenge: the calcium–vitamin D balance can be thrown off by physiology, diet, kidney function, or even confusing lab patterns. Let’s untangle how PTH choreographs the relationship between calcium and vitamin D, and why the plot can thicken unexpectedly.
Meet the Parathyroid Hormone: The Body’s Calcium Emergency Dispatcher
Parathyroid hormone is secreted by the parathyroid glands, typically four small glands tucked behind the thyroid. Its primary directive is elegantly simple: maintain serum calcium within a narrow, life-compatible range.
When calcium levels fall—whether due to low intake, poor absorption, increased losses, or vitamin D insufficiency—PTH rises. It’s not dramatic for the sake of drama; it’s protective, acting like a homeostasis thermostat. The body must keep calcium available for neuromuscular transmission, muscle contraction, cardiac rhythm stability, and myriad cellular signaling pathways.
Yet the body doesn’t respond with a single lever. PTH orchestrates multiple routes at once: it influences bone turnover, renal calcium handling, and the activation of vitamin D. This multi-pronged approach is what makes PTH such a powerful mediator—and why misfires can create complex downstream effects.
Calcium Drops: What Triggers PTH to Rise?
Calcium sensing is central. When ionized calcium in the bloodstream decreases, the parathyroid glands interpret the change and increase PTH secretion. This response can occur quickly. Sometimes it’s subtle; sometimes it’s obvious after dietary limitations, malabsorption syndromes, or certain medications.
Vitamin D deficiency can create a domino effect. Without adequate vitamin D, intestinal absorption of calcium weakens. The body then compensates by increasing PTH, which tries to restore calcium availability. This is where the “potential challenge” sneaks in: high PTH might look like an isolated abnormality, but it can be the compensatory signature of a broader imbalance—especially an inadequate vitamin D status.
PTH and the Kidney: Reclaiming Calcium Like a Recycling Machine
The kidneys are a key battleground for calcium economy. One of PTH’s major actions is to reduce urinary calcium loss by increasing calcium reabsorption in the renal tubules.
In practical terms, PTH tells the kidneys: “Stop letting calcium escape.” This conserves serum calcium and supports normal physiologic function. But the kidney doesn’t only handle calcium—it also manages phosphate. PTH tends to decrease phosphate reabsorption, which leads to increased phosphate excretion in urine.
This trade-off is not random. Phosphate dynamics matter because calcium and phosphate can precipitate under certain conditions. The endocrine system navigates the fine line between availability and biochemical stability.
Long sentences have their place, but the idea is straightforward: PTH tightens calcium retention while loosening phosphate grip.
PTH and Vitamin D Activation: Converting Inactivity to Usefulness
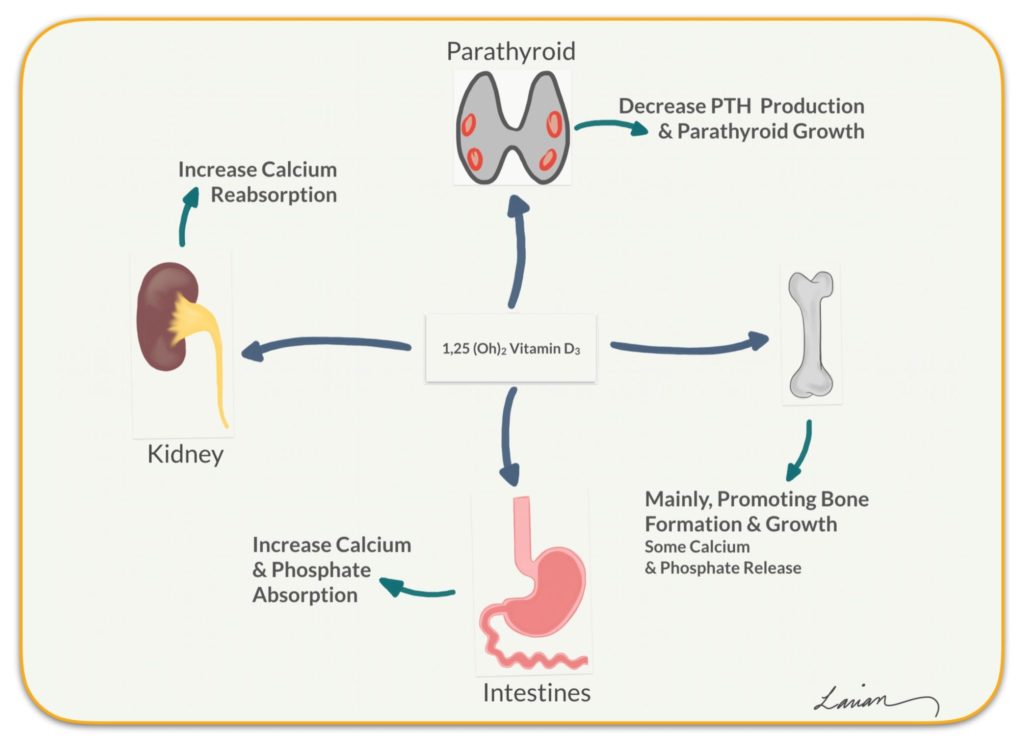
Vitamin D isn’t automatically “active” just because it exists in the body. Many forms must undergo conversion. PTH helps by stimulating the renal 1-alpha hydroxylase enzyme, which converts 25-hydroxyvitamin D into the more active 1,25-dihydroxyvitamin D (calcitriol).
Calcitriol then boosts intestinal calcium absorption—an important step in restoring calcium levels when they fall due to inadequate dietary intake or reduced absorption efficiency.
Here’s where the narrative becomes fascinating: PTH doesn’t merely raise calcium through kidney effects; it also “primes” the system for better absorption by activating vitamin D. In other words, PTH helps vitamin D become operational, not merely present.
If vitamin D stores are low, PTH can only do so much. The enzyme machinery may be stimulated, but there may not be sufficient substrate (the precursor vitamin D) to generate enough active calcitriol. This limitation can intensify metabolic confusion and contribute to persistent biochemical abnormalities.
PTH and Bone: The Quiet Remodeling That Can Become Loud
Bone is not a static warehouse. It is living tissue with constant remodeling. PTH influences this process, and its effects can vary depending on whether PTH is elevated continuously or intermittently.
When PTH is chronically high, it generally promotes increased bone resorption, releasing calcium and phosphate into circulation. This can be helpful in the short term to restore serum calcium. But over time, sustained PTH elevation may weaken bone integrity and contribute to osteopenia or osteoporosis.
Bone is where the body’s “backup supply” lives. The challenge is that using it too heavily or for too long can create structural consequences. Think of it like repeatedly tapping a savings account—at first it keeps things afloat; later, the account balance runs thin.
Conversely, intermittent PTH stimulation (as in certain medical therapies) can support bone formation more than resorption. That nuance highlights why PTH is not inherently harmful—it’s the pattern and context that matter.
Phosphate: The Often-Ignored Co-Star in the Calcium Story
Calcium and phosphate share a biochemical relationship that resembles two musicians coordinating in a duet. PTH tends to lower serum phosphate by increasing phosphate excretion. This helps make more calcium available and modulates mineral balance.
However, phosphate doesn’t just disappear. Its levels reflect intake, absorption, kidney handling, and cellular shifts. When vitamin D is activated by PTH, phosphate absorption in the gut can also increase. So, while PTH lowers phosphate reabsorption in the kidney, calcitriol may enhance intestinal phosphate uptake.
This creates a web of cause-and-effect where lab results can appear contradictory if you don’t consider the timeline and the endocrine feedback loops.
What Happens When Vitamin D and PTH Fall Out of Sync?
Imagine vitamin D is the “fuel,” while PTH is the “instructor” trying to make the body use the fuel effectively. If vitamin D stores are low, the instructor can increase the activation signal, but the classroom may still lack enough textbooks. Calcium absorption may remain insufficient.
In that scenario, PTH can become persistently elevated as compensation. This may lead to increased bone turnover and symptoms that can be mistaken for unrelated issues—muscle weakness, bone pain, fatigue, or even tingling sensations if calcium becomes low enough.
Another layer of complexity emerges when kidney function is reduced. The kidney is central for vitamin D activation. If activation falters, PTH may rise even when vitamin D intake exists, resulting in an imbalance that looks like “vitamin D deficiency” from the perspective of physiology but behaves differently in underlying cause.
Symptoms, Lab Clues, and Why the Pattern Matters
Clinicians often interpret PTH in relation to calcium, phosphate, and vitamin D levels rather than in isolation. A single elevated number rarely tells the whole story. Patterns are the key.
If calcium is low or low-normal with elevated PTH, compensation is likely. If calcium is high with elevated PTH, the story shifts toward a different mechanism. If vitamin D is low, PTH may be elevated as an understandable response to inadequate absorption and activation.
That’s why the potential challenge is real: people may focus on one number and miss the orchestration. The endocrine system works in concert, and the lab panel is like a snapshot—useful, but incomplete without context.
Visualizing the Feedback Loop: How PTH, Calcium, and Vitamin D Interact
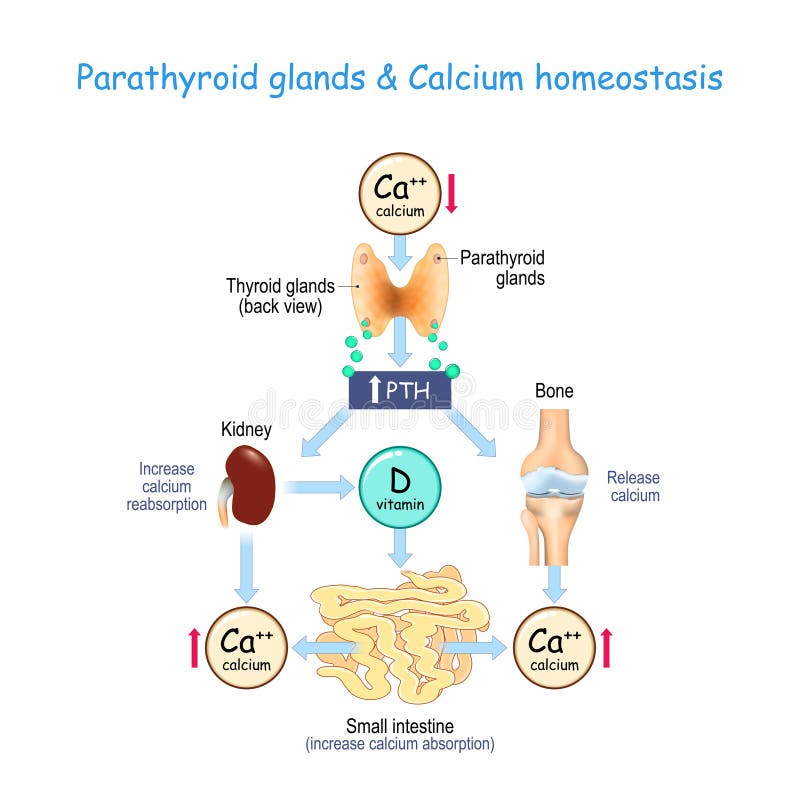
It can help to picture a feedback loop. When calcium drops, PTH rises. PTH then increases renal calcium retention, mobilizes calcium from bone, and activates vitamin D. Active vitamin D enhances intestinal calcium absorption, bringing calcium back toward target levels. Meanwhile, phosphate handling shifts in response to maintain mineral equilibrium.
If any component is impaired—insufficient vitamin D stores, limited kidney activation, or chronic hormonal overstimulation—the loop becomes uneven. The result can be persistent elevation of PTH, altered mineral balance, and downstream effects on bones and muscles.
Practical Implications: The Real-World Challenge of Correcting the Loop
Correcting calcium–vitamin D imbalance isn’t just about “adding more vitamin D” and hoping everything resolves. The body’s response depends on the cause: dietary insufficiency, malabsorption, medication effects, kidney function, or parathyroid gland dysregulation.
Sometimes vitamin D repletion lowers PTH by restoring calcium absorption. Sometimes it improves the substrate but not the activation pathway. And sometimes PTH elevation reflects a primary parathyroid issue rather than merely inadequate vitamin D.
Thus, the most effective strategy is usually guided by a coherent plan: measure the relevant markers, identify the pattern, and address the root constraint. The goal is not only normalization of labs, but stabilization of mineral homeostasis over time—so the ringmaster can step back to a calm, steady rhythm.
When to Take the Question Seriously: A Closing Playful Note
So, here’s the playful question again: what if your body’s “compensation” is working… but it’s still not enough? When PTH remains elevated, it may be both a helpful response and a warning sign. The calcium–vitamin D balance is a dynamic negotiation, and PTH is the referee who can’t change the rules—only interpret them.
If symptoms suggest metabolic imbalance or if lab patterns show discord between vitamin D, calcium, and PTH, it’s worth pursuing a structured evaluation. The reward is clarity: understanding whether the loop is starved of fuel, blocked by infrastructure, or driven by an endocrine miscommunication.