
It’s a curious irony: vitamin D—the nutrient so often celebrated for its role in bones and immune modulation—can, in excess, become a spark that ignites a very specific kind of danger. Hypercalcemia, the elevation of calcium in the bloodstream, is frequently treated as though it arrives from nowhere, yet it often has a biochemical trail that loops back to vitamin D. The link is not merely theoretical; it is mechanistic, patient-specific, and sometimes surprisingly easy to overlook. And once you see the pathway, the fascination becomes almost unavoidable: how can something designed to protect skeletons end up disturbing the very calcium equilibrium it helps regulate?
Why hypercalcemia seems “unexpected” in the vitamin D story
A common observation is that hypercalcemia feels like an “outside” problem—something driven by malignancy, parathyroid disorders, or mysterious metabolic syndromes. Meanwhile, vitamin D is often regarded as a safe, everyday supplement. That perception can blur clinical vigilance. Many people dose vitamin D for long periods without fully appreciating how slowly vitamin D metabolites accumulate or how individual physiology alters conversion and clearance.
The deeper reason for the surprise is that calcium is not a simple nutrient equation. It is a tightly choreographed variable governed by bone turnover, renal handling, intestinal absorption, and hormonal signals. When vitamin D intoxication occurs, it doesn’t just raise calcium—it reconfigures the hormonal “rules of the game,” and the bloodstream interprets that reconfiguration as permission to flood the system with calcium.
The biochemical hinge: vitamin D’s effect on intestinal calcium absorption
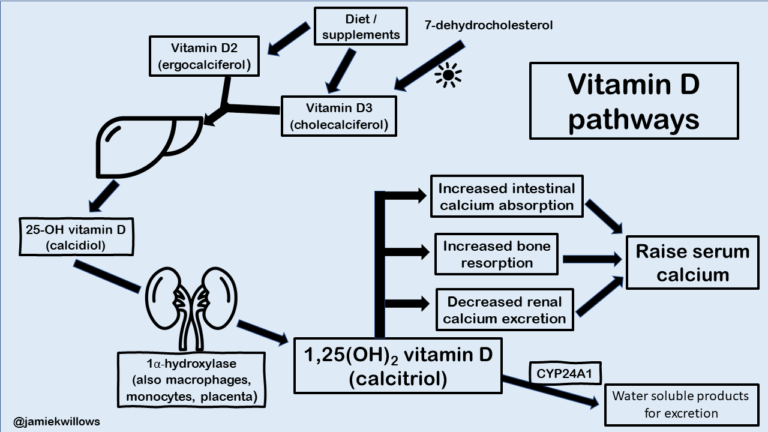
Vitamin D’s most famous job is facilitating calcium absorption in the gut. Normally, this absorption is calibrated. It increases when the body senses insufficient mineral availability and is moderated when calcium stores are adequate.
In toxicity, that moderation falters. Elevated vitamin D leads to higher levels of active metabolites, which act like over-amplified transcription factors for calcium-transport machinery. Think of the intestinal lining as a turnstile: in health, it admits calcium at a measured rate; in toxicity, it becomes permissive to the point of excess.
The result is a sustained rise in serum calcium that can persist even after typical dietary changes. A person may consume “only” supplements, yet their blood calcium begins behaving as though they ingested far more calcium than they actually did.
Hypercalcemia’s downstream ripple: kidneys, bones, nerves, and fatigue
When serum calcium climbs, multiple organ systems receive the message that the internal environment has become mineral-rich. The kidneys attempt to compensate by increasing urinary calcium excretion, but high calcium loads can also impair the kidney’s ability to maintain fluid balance.
Clinically, this cascade can present as thirst, frequent urination, constipation, abdominal discomfort, and a persistent sense of lassitude. Neuromuscular symptoms—ranging from weakness to confusion in severe cases—may appear because calcium modulates nerve excitability. Even cardiac rhythms can be affected when calcium levels become markedly abnormal.
Bones, meanwhile, are paradoxically drawn into the story. In many hypercalcemia states, bone resorption increases, releasing calcium from the skeleton into circulation. Vitamin D intoxication can tilt the balance toward more resorption and less orderly mineral maintenance, so the body ends up “selling” calcium to the blood that later causes the problem.
What counts as vitamin D toxicity: forms, timing, and the role of active metabolites
Vitamin D intoxication is not always the result of a single mega-dose. It can develop gradually after repeated high intake, particularly with products that deliver large bolus amounts or with dosing that exceeds individualized requirements.
Another nuance: the body does not treat all vitamin D pathways identically. Some individuals convert vitamin D to active metabolites more efficiently or clear them more slowly. Others may have underlying conditions that alter vitamin D metabolism. Consequently, two people taking the same regimen may produce different calcium trajectories.
There is also a conceptual distinction between “high vitamin D levels” and the most clinically relevant factor: the downstream activation of calcium-absorptive pathways. The body can accumulate precursors, and the excess converts into active forms, generating hypercalcemia as a later consequence rather than an immediate event.
When the parathyroid axis goes quiet: suppressed PTH and the hormonal signature
One of the most informative clinical clues is parathyroid hormone (PTH). Under normal conditions, when calcium rises, PTH secretion decreases. This is homeostatic logic: the parathyroids sense abundant calcium and reduce their signal.
In vitamin D–induced hypercalcemia, PTH is typically suppressed. That suppression helps distinguish vitamin D toxicity from hypercalcemia driven by primary hyperparathyroidism or other PTH-mediated causes. The hormonal signature acts like a biochemical fingerprint: the body is reacting correctly to high calcium, but the upstream cause remains overpowering.
This is part of the fascination: the endocrine system becomes a witness, recording its own conclusions through laboratory patterns.
Hypercalcemia can look like other disorders—until you trace the pattern
Because hypercalcemia is a final common pathway for multiple etiologies, it can initially resemble other diagnoses. Cancer-related mechanisms, granulomatous disease, medication effects, and inherited disorders can all raise calcium through distinct routes.
Vitamin D toxicity, however, tends to show a consistent alignment: elevated vitamin D metabolites (particularly the active fraction or the relevant precursor, depending on what is measured) and suppressed PTH. Sometimes phosphate patterns shift as well, reflecting changes in hormonal regulation and renal handling.
Radiologic or symptom-based impressions may be misleading, because the body’s end-stage response—fatigue, dehydration, gastrointestinal distress—does not uniquely identify vitamin D. The deeper reason to look for the biochemical pattern is that the mechanism directs the cure.
Impaired clearance and vulnerable groups: who is more at risk
Some populations appear to stand on a higher-pressure line. Chronic kidney disease can reduce the body’s ability to handle calcium and related metabolic processes. Certain medications can alter vitamin D metabolism or calcium balance. Malabsorption syndromes, autoimmune conditions, or granulomatous disorders may amplify the conversion of vitamin D into active forms through pathways not strictly regulated like normal physiology.
Older adults are often particularly vulnerable—not because their bodies are weaker in a simplistic sense, but because dosing practices and comorbidity profiles increase the likelihood of unintended accumulation. The same supplement regimen can behave differently depending on hydration status, renal function, and concurrent therapies.
Risk is rarely a single-factor story. It is usually a convergence: higher exposure plus reduced buffering capacity plus delayed recognition.
The role of granulomatous disease: vitamin D metabolism “out of rhythm”
There is also an intriguing overlap between vitamin D physiology and conditions involving immune activation. In some granulomatous diseases, cells in the affected tissue can produce active vitamin D metabolites in an unregulated manner. In those settings, the body effectively manufactures active vitamin D where it normally would not.
This can produce hypercalcemia even without massive supplementation. Yet supplementation may exacerbate the problem. The result is that vitamin D excess and vitamin D dysregulation can merge, creating a snowball effect: absorption and activation reinforce each other.
Thus the link between vitamin D toxicity and hypercalcemia is not only about “taking too much.” It is also about the body’s regulatory circuitry sometimes being hijacked.
Clinical management: removing the spark and restoring equilibrium
When hypercalcemia is attributed to vitamin D intoxication, management typically begins with stopping vitamin D intake and addressing hydration status. Because calcium levels reflect both intake-derived absorption and bodily handling, restoring renal perfusion and encouraging urinary calcium excretion often becomes central.
In more severe cases, clinicians may use additional therapies to lower calcium and protect organ function. The exact strategy depends on severity, symptoms, kidney function, and the measured metabolite pattern.
Importantly, recovery can take time. Vitamin D metabolites are fat-soluble, and their residence time in the body can prolong the hypercalcemic phase even after supplementation is discontinued. Patience becomes a therapeutic component, paired with monitoring to ensure the calcium level declines safely.
Prevention: the quiet discipline behind “safe dosing”
Prevention is often more about humility than heroism. Vitamin D is not a one-size-fits-all supplement. Dosing should consider baseline vitamin D status, absorption capacity, body weight considerations, renal function, and concurrent medical conditions.
Monitoring—especially in people receiving higher doses or long-term supplementation—helps identify early drift toward toxicity. Symptoms can be nonspecific, and by the time hypercalcemia is obvious, the biochemical overrun may have already extended for weeks or months.
A practical prevention mindset resembles calibration of instruments. Rather than assuming that “more” equals “better,” it treats vitamin D like a precision variable: useful in correct proportions, disruptive in excess.
Images that capture the concept: calcium’s gravity and the skeleton key metaphor
Hypercalcemia is not only a lab abnormality; it is a shift in physical chemistry that reverberates through the body’s systems. In visual form, the “gravity” of calcium becomes intuitive—once calcium floods the bloodstream, it seeks new balances everywhere, from renal handling to neuromuscular excitability.


The lasting takeaway: the link is a pathway, not a coincidence
The fascination in vitamin D toxicity and hypercalcemia lies in how elegantly the body connects distant processes. A nutrient that improves calcium absorption can become, in excess, the very force that distorts calcium homeostasis. The endocrine system may respond appropriately by suppressing PTH, yet that very suppression is part of the story: it signals that the problem is upstream and overpowering.
When hypercalcemia appears, it should not be viewed as an isolated catastrophe. It is often a readable consequence of mechanism—sometimes driven by medications or disease, and sometimes by a supplement taken with good intentions. Understanding the link transforms uncertainty into a map, and a map makes prevention and treatment far more achievable.



