Vitamin D has a peculiar talent for slipping into the background—until it suddenly becomes the story. After bariatric surgery, that “quiet” nutrient can behave differently, and the body’s ability to harvest it may feel like it has been redesigned overnight. The result is not only a medical question but also a shift in perspective: vitamin D absorption isn’t merely about eating the right foods or taking supplements. It is also about anatomy, chemistry, time, and the choreography of digestion itself. And once you begin to look at it that way, curiosity turns inevitable—because what seems like a straightforward deficiency can be a window into the body’s deeper adaptations.
Why Vitamin D Absorption Is So Sensitive
Vitamin D is fat-soluble, meaning it prefers to travel alongside lipids rather than moving freely in watery pathways. That matters because absorption is not a single event—it’s a sequence. Dietary fat enters the small intestine, bile acids emulsify fat into smaller droplets, and intestinal enzymes and transport processes help liberate nutrients for uptake. Vitamin D, tucked inside this lipid world, depends on smooth digestive mechanics.
So when the digestive system is altered surgically, the “routing” of absorption can change. The intestine may still do its job, but the timing and location of digestion may shift. Even small deviations in the environment—like bile availability, the length of contact time, or intestinal surface area—can create a domino effect. This is why some individuals sail through surgery with minimal vitamin D disruption, while others experience a slow, insidious decline.
The Surgical Landscape: Malabsorptive vs. Restrictive Changes
Bariatric procedures are not all the same, and vitamin D outcomes often mirror that distinction. Restrictive techniques primarily limit stomach capacity, altering how much food can be consumed. Malabsorptive techniques, on the other hand, can reduce how much of the ingested material is exposed to the intestinal absorptive surfaces.
Roux-en-Y gastric bypass, for example, reroutes food so it bypasses parts of the upper small intestine. This can shorten the effective “processing route” for nutrients like vitamin D. Sleeve gastrectomy tends to be more restrictive, but it still influences gastric physiology and downstream signaling. Gallbladder function, bile flow patterns, and changes in intestinal transit time can all contribute, even when the procedure is not primarily malabsorptive.
In other words, the body’s response is architectural and dynamic. The question becomes: where does vitamin D encounter the conditions it needs to be absorbed efficiently?
Mechanisms After Surgery: Where the Chain Gets Looser
To understand the effect of bariatric surgery on vitamin D absorption, it helps to zoom in on the absorption chain and notice which links are most vulnerable.
First, bile dynamics may be altered. Bile acids are central to fat emulsification. If fat processing changes, vitamin D—being fat-soluble—may be less effectively packaged into absorbable forms.
Second, intestinal surface area and exposure time can decrease. If the absorptive window is shorter, vitamin D has less time to cross into circulation.
Third, fat intake and dietary behavior often change. Many patients reduce overall fat consumption early on. Even if vitamin D is present, less lipid movement can reduce the “vehicle” needed for solubilization.
Fourth, inflammatory and hormonal shifts can interfere indirectly. After surgery, changes in gut hormones and immune signaling may influence nutrient handling. It is not always a direct mechanical failure; sometimes the environment becomes less cooperative.
The Timeline of Deficiency: Not Always Immediate, Not Always Obvious
Vitamin D deficiency after bariatric surgery rarely announces itself with a single dramatic event. Instead, it often emerges gradually. Early months may be dominated by recovery, dietary transitions, and altered absorption patterns. Then, as supplementation routines evolve—or as adherence fluctuates—levels may drift downward.
Some people feel fine while their vitamin D stores quietly decline. Others notice musculoskeletal discomfort sooner than lab results confirm. This is where perspective shifts again: symptoms can lag behind biochemistry, and biochemistry can change before symptoms become meaningful.
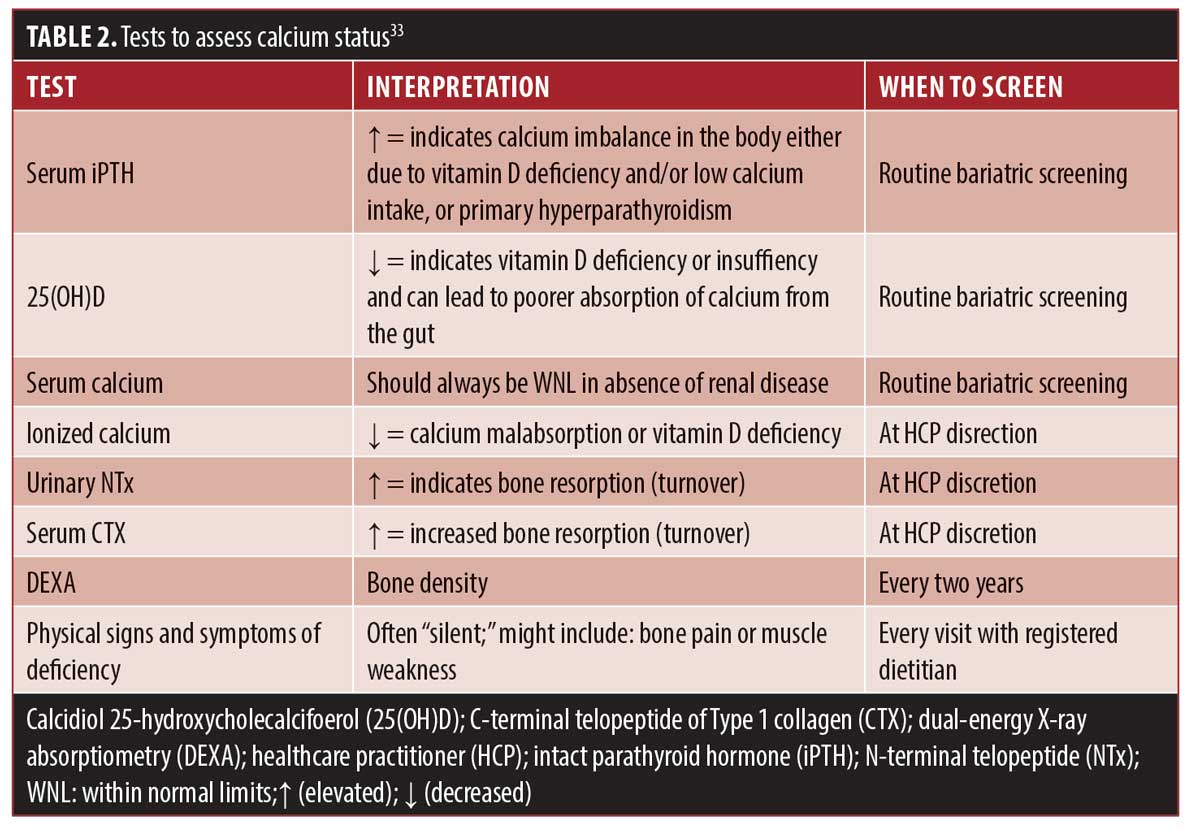
Regular monitoring becomes the compass. Blood tests—particularly 25-hydroxyvitamin D—help reveal what the body is actually doing, not just what it seems to be doing.
Calcium, Parathyroid Hormone, and the Indirect Pressure on Bone
Vitamin D rarely works alone. It partners with calcium to support mineralization of bone. When vitamin D absorption decreases, calcium absorption can also fall. The body compensates by increasing parathyroid hormone (PTH), which acts like a regulator that shifts the balance to protect blood calcium levels.
High PTH can lead to increased bone resorption over time. That is a crucial pivot point in the narrative: the problem is not only low vitamin D in a lab report. It is the downstream risk to skeletal integrity—particularly in individuals already predisposed to bone loss.
So the effect of bariatric surgery on vitamin D absorption can be understood as an upstream event with downstream consequences, moving from absorption → deficiency → hormonal compensation → bone remodeling.
How Supplementation Fits In: A New Strategy, Not a Simple Addition
Many patients assume that taking vitamin D supplements is a straightforward fix. Yet the post-surgical landscape can make “normal dosing” insufficient. If absorption efficiency is altered, the body may require different forms, higher doses, or more consistent administration patterns.
Supplementation strategies often include oral vitamin D preparations, sometimes paired with calcium. Some clinicians may consider higher-dose regimens or more targeted schedules depending on lab results. The key point is that supplementation is not merely a pill—it is a calibrated response to altered digestion.
And there’s another layer of curiosity: the form of vitamin D matters. Some individuals respond better to certain formulations, while others need adjustments based on measured levels over time.
Why Lifestyle and Diet Still Matter (Even After Surgery)
After bariatric surgery, food becomes both medicine and data. Vitamin D absorption may be biologically constrained, but diet and routine still influence overall vitamin status.
Fat intake, for instance, can affect solubilization of fat-soluble nutrients. Too little dietary fat may reduce absorption opportunities; too much may conflict with nutritional goals or tolerance. Similarly, sun exposure can influence vitamin D stores, though it varies widely by geography, season, skin pigmentation, and behavior.
Exercise also nudges the story forward. Weight-bearing activity supports bone health and may counterbalance some skeletal risks associated with deficiency-driven hormonal changes.
Interpreting Lab Results: The Body’s Hidden Accounting
Laboratory values are an imperfect mirror of lived experience, yet they are essential for navigating post-surgical nutrition. Vitamin D status is often assessed via 25-hydroxyvitamin D, which reflects circulating stores. Calcium and PTH provide additional context, revealing whether the body is compensating.
If vitamin D is low and PTH is elevated, that combination signals physiological urgency. It suggests the body is doing what it must to maintain calcium in the bloodstream, even if the cost is paid in bone remodeling. This is the moment where numbers become narrative.
Monitoring transforms uncertainty into a plan: adjusting supplements, timing administration, and aligning nutritional intake with the altered anatomy of absorption.
Common Pitfalls: The Quiet Reasons Levels Stay Low
Even with good intentions, vitamin D deficiency can persist after surgery. One pitfall is inconsistent supplement adherence—particularly when early follow-up becomes less frequent. Another is inadequate follow-up testing, which can delay correction of declining levels.
Some patients experience intolerance to supplements or have difficulty maintaining dietary patterns during stress, travel, or changing health circumstances. There can also be variations in absorption related to procedure type, individual anatomy, concurrent conditions, and medication interactions.
These are rarely dramatic errors. They are often subtle, cumulative factors. And that’s exactly why ongoing guidance and periodic assessment matter.
A Forward-Looking Perspective: Protection Through Personalization
The effect of bariatric surgery on vitamin D absorption is not a simple verdict. It’s a conversation between altered anatomy and nutrient biology. The body adapts, but adaptation does not always preserve optimal vitamin D status without support.
What ultimately offers reassurance is personalization: matching dosing and monitoring to the individual’s lab patterns, procedure type, dietary realities, and lifestyle. When vitamin D absorption is treated as a dynamic system rather than a static rule, outcomes improve—and curiosity turns into confidence.
In the end, vitamin D after bariatric surgery is not just about deficiency. It is about stewardship of bone health, endocrine balance, and long-term resilience. Once that perspective takes root, the pathway forward becomes clearer.