
There is a particular kind of sunlight memory that pregnancy invites—an almost instinctive faith that what nourishes the outside world can also nurture the body within. Yet beneath that comforting belief lies a quieter truth: vitamin D is not merely a “bone vitamin.” It behaves more like a molecular diplomat, negotiating between immune signals, vascular health, and cellular inflammation. When that dialogue falters, pregnancy can become more complicated than expected. Preeclampsia, in particular, may be one of the conditions where vitamin D’s influence becomes visible—sometimes early, sometimes late, and often in ways that surprise even attentive clinicians and families.
Vitamin D in Pregnancy: More Than a Nutrient
Vitamin D’s headline role is often described as calcium regulation and skeletal strength. But in pregnancy, it undertakes a broader assignment. It helps modulate immune tolerance, supports endothelial function (the “lining” of blood vessels), and participates in the regulation of inflammatory pathways. This matters because pregnancy is, by design, an immunologically sophisticated process. The maternal body must adapt without rejecting the developing fetus, and blood vessels must transform to accommodate increasing demands.
When vitamin D levels are suboptimal, the immune system may become less balanced—less “harmonized,” more reactive. In parallel, the vascular network may become less responsive. Think of it as a finely tuned orchestra where one instrument is slightly off-key. The performance still happens, but the music carries an undertone of risk.
Preeclampsia Unveiled: Why Blood Vessels Become the Plot
Preeclampsia is not a single symptom—it is a vascular story with systemic echoes. It often emerges after impaired placental development leads to abnormal maternal vascular responses. Blood vessels can fail to dilate properly, and inflammatory mediators may surge. The result can include hypertension, proteinuria, and organ stress. Some pregnancies experience preeclampsia early, others later, and the timing can influence the pattern of complications.
Here is where vitamin D’s potential relevance sharpens. If endothelial function and inflammatory control are part of the preeclampsia narrative, then vitamin D—an orchestrator of both—becomes a variable worth considering. Not as a magic fix. Not as a guarantee. But as a meaningful piece of the puzzle.
Early-Onset vs Late-Onset: Different Rhythms, Different Vulnerabilities
Pregnancies are not monolithic. Early-onset preeclampsia (often defined as occurring before a certain gestational threshold) can reflect more profound placental dysfunction and may be associated with more severe disease trajectories. Late-onset preeclampsia may still be serious, yet the mechanism can differ, involving a more gradual accumulation of stressors.
Vitamin D’s relationship to both forms may not be identical, but the underlying themes overlap: inflammation, immune balance, and vascular performance. If vitamin D insufficiency correlates with impaired regulation, then the earliest, most fragile pregnancies may be more likely to show the consequences of that imbalance.
Curiosity is warranted here. Could improving vitamin D status create more “room” for placental adaptation? The question is not trivial, and it invites a shift in perspective—from viewing preeclampsia as unforeseeable fate to seeing it as a condition influenced by modifiable biology.
Pathways of Concern: Inflammation, Endothelial Dysfunction, and Immune Tuning
Imagine pregnancy as a high-stakes construction project occurring under strict time pressure. Placental development requires controlled remodeling of blood vessels. Vitamin D participates in the signaling that helps regulate this remodeling process. It can influence cytokines—chemical messengers that can either calm inflammation or amplify it.
Endothelial dysfunction is another critical thread. The endothelium helps control vascular tone and blood flow. When it becomes dysfunctional, the cardiovascular system may respond with exaggerated constriction and impaired perfusion. That can set the stage for the hypertension and systemic effects that characterize preeclampsia.
Then there is immune tuning: pregnancy requires a delicate immunological negotiation. Vitamin D is implicated in promoting an immune environment compatible with fetal development. When that environment becomes skewed, placental and maternal interactions may tilt toward pathology.
Risk Factors and the Vitamin D Overlap: What Often Travels Together
Preeclampsia risk is influenced by many variables: first pregnancy, age extremes, chronic hypertension, preexisting metabolic conditions, kidney disease, and certain placental-related factors. Many of these risks also intersect with lifestyle and nutritional determinants. Vitamin D insufficiency is more likely in situations such as limited sun exposure, darker skin pigmentation under low ultraviolet conditions, higher body mass index (due to vitamin D sequestration in adipose tissue), and dietary patterns that provide little vitamin D.
This overlap matters because it suggests that vitamin D status may act as a “context signal.” It doesn’t replace the major risk factors—but it may modulate susceptibility. In other words: two pregnancies can share similar clinical profiles, yet vitamin D may influence how the system copes under stress.
What Low Vitamin D Can Look Like: Symptoms Are Not the Full Story
Low vitamin D rarely announces itself with a single unmistakable symptom. Fatigue, generalized aches, or subtle mood changes may occur, but these are common in pregnancy regardless of vitamin D status. That ambiguity can create a false sense of certainty: “I feel fine, so my levels must be fine.” The biology doesn’t always follow that logic.
Laboratory testing is the only way to truly illuminate the picture. Even then, interpretation depends on trimester context and local reference ranges. The key point is simple: absence of obvious symptoms does not equal absence of deficiency.
Testing and Thresholds: Choosing Clarity Over Guesswork
Clinical care often involves measuring 25-hydroxyvitamin D, a marker that reflects vitamin D stores. Yet thresholds for sufficiency can vary between guidelines. The practical takeaway is that testing transforms vitamin D from a vague wellness concept into an actionable clinical variable.
If vitamin D insufficiency is identified, the next step is not panic. It is personalization: discussing supplementation plans with a healthcare professional who can account for prenatal vitamins, dietary intake, pregnancy-specific risk, and overall health.
Supplementation Possibilities: A Measured Approach, Not a Sweepstakes
Vitamin D supplementation is commonly used during pregnancy. The central principle is titration: dosing that matches deficiency severity while maintaining safety. Supplement regimens often consider baseline levels and may be adjusted over time. Some clinicians recheck levels later to confirm response.
There is also a broader lifestyle dimension—safe sun exposure, dietary sources, and consistent prenatal nutrition. However, pregnancy can limit how realistically those supports can be optimized, especially during seasons with low ultraviolet intensity or in regions where sunlight is scarce.
Here, the shift in perspective is powerful: instead of treating vitamin D as an optional lifestyle add-on, consider it a structured variable within prenatal risk management—one that may help the body maintain vascular and immune resilience.
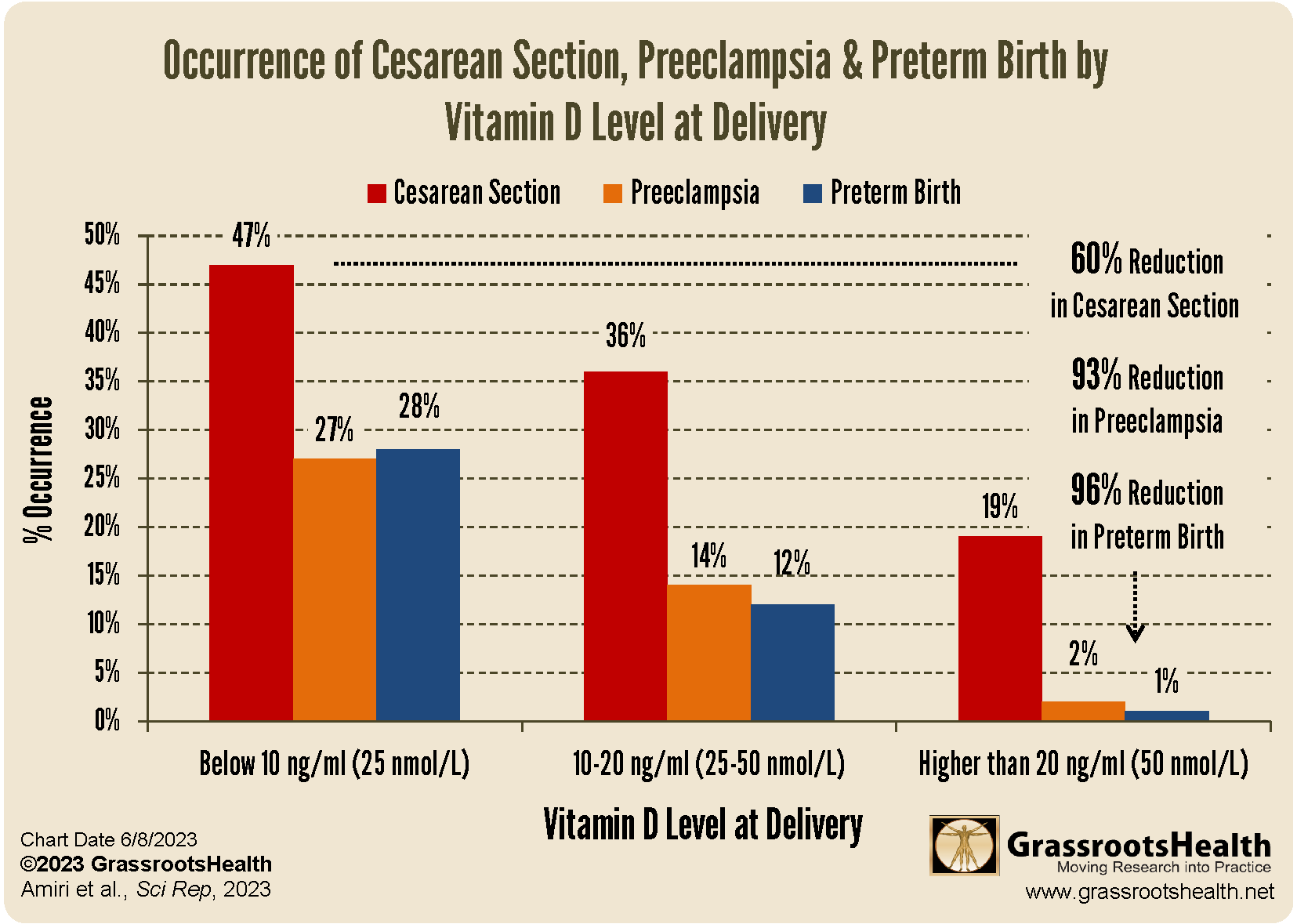
Cesarean Section, Preterm Birth, and the Ripple Effects of Complications
Preeclampsia does not exist in isolation. It can influence delivery decisions and neonatal outcomes. When preeclampsia becomes severe or threatens maternal-fetal health, clinicians may recommend earlier delivery, sometimes via cesarean section. Preterm birth can follow, and the downstream implications—NICU exposure, feeding challenges, developmental monitoring—can reshape the entire early life narrative.
While vitamin D is not a standalone explanation for obstetric outcomes, the possibility of association invites reflection: if vitamin D status relates to preeclampsia risk, then it may indirectly connect to downstream complications. The goal is not determinism. It is prevention-minded awareness.
Nutrition Patterns and Vitamin D Synergy: The Body’s Whole-System Language
Vitamin D rarely works alone. It interacts with calcium intake, magnesium metabolism, overall protein adequacy, and inflammatory balance. A pregnancy diet rich in micronutrients may support the downstream systems vitamin D influences. Conversely, nutritional constraints—iron deficiency, inadequate protein, low intake of fat-soluble vitamin sources—can complicate the response.
In practical terms, supplementation is most meaningful when paired with a nutrition strategy that supports vascular health: a balance of energy and macronutrients, adequate hydration, and attention to dietary diversity. The body responds best when it receives a coherent biochemical message rather than isolated supplements.
When to Have the Conversation: Timing Matters
Timing is not just about when symptoms appear. It is about when vitamin D status is addressed. Early pregnancy is often a window when placental adaptation begins in earnest. Addressing potential deficiency early can be part of a proactive strategy.
Still, late pregnancy conversations can be valuable too. If deficiency is discovered later, correcting it may help support ongoing physiological needs, though the degree of influence may vary by disease trajectory.
A Curiosity-Driven Conclusion: Reframing Risk as Biology You Can Influence
Preeclampsia can feel like a storm that arrives without warning. But the more deeply pregnancy is understood, the more it resembles a system that communicates in signals—some of which are influenced by nutrition and immune-vessel interactions. Vitamin D sits at an interesting intersection of those signals: inflammation, endothelial function, and immune tolerance.
Rather than treating vitamin D as a vague wellness theme, consider it a measurable biological variable. Test when appropriate. Discuss supplementation thoughtfully. Align diet and lifestyle with safe, evidence-aware strategies. Above all, let the conversation be grounded in curiosity—because curiosity changes how people prepare. And when preparation is informed by biology, risk management becomes less about fear and more about agency.
Further Reading Options
If you enjoy digging into the evidence landscape, these materials can help contextualize the vitamin D–preeclampsia conversation and explore how risk factors may vary by timing of onset.






